

Comorbidities and complications of COVID-19 associated with disease severity, progression, and mortality in China with centralized isolation and hospitalization: A systematic review and meta-analysis
- PMID: 36052001
- PMCID: PMC9424916
- DOI: 10.3389/fpubh.2022.923485
Comorbidities and complications of COVID-19 associated with disease severity, progression, and mortality in China with centralized isolation and hospitalization: A systematic review and meta-analysis
Abstract
Background: Coronavirus disease 2019 (COVID-19) causes life-threatening with the high-fatality rates and spreads with high-infectious disease worldwide. We aimed to systematically review the comorbidities and complications of COVID-19 that are associated with various disease severity, progression, and mortality in China, to provide contemporary and reliable estimates in settings with centralized isolation and hospitalization.
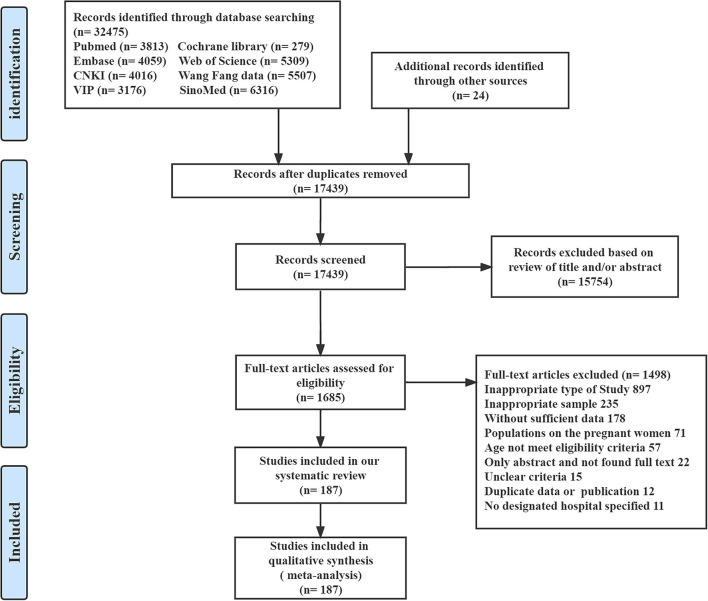
Methods: In this systematic review and meta-analysis, we searched four main English language databases, and four main Chinese language databases for observational studies published from inception to January 2022, to identify all the related comorbidities and complications of COVID-19, in the China region with centralized isolation and hospitalization, with disease severity, progression, and mortality. Literature search, data extraction, and quality assessment were independently conducted by two reviewers. We used the generalized linear mixed model to estimate pooled effect sizes for any comorbidities and complications, and subgroup in gender ratio was done to further address the potential heterogeneity.
Results: Overall, 187 studies describing 77,013 patients, namely, 54 different comorbidities and 46 various complications of COVID-19, were identified who met our inclusion criteria. The most prevalent comorbidities were hypertension [20.37% 95% CI (15.28-26.63), 19.29% (16.17-22.85), 34.72% (31.48-38.10), and 43.94% (38.94-49.06)] and diabetes [7.84% (5.78-10.54), 8.59% (7.25-10.16), 17.99% (16.29-19.84), and 22.68% (19.93-25.69)] in mild, moderate, severe, and critical cases. The most prevalent complications were liver injury [10.00% (1.39-46.72), 23.04% (14.20-35.13), and 43.48% (39.88-47.15)] in mild, moderate, and severe cases, and acute respiratory distress syndrome [ARDS; 94.17% (20.78-99.90)] and respiratory failure [90.69% (28.08-99.59)] in critical cases. Renal insufficiency [odds ratio (OR) 17.43 (6.69-45.43)] in comorbidities and respiratory failure [OR 105.12 (49.48-223.33)] in complications were strongly associated in severe/critical than in mild/moderate cases. The highest estimated risk in intensive care unit (ICU) admission, progression, and mortality was an autoimmune disease, nervous system disease, and stroke in comorbidities, shock, and ARDS in complications.
Conclusion: Comorbidities and complications in inpatients with COVID-19 were positively associated with increased risk in severe and critical cases, ICU admission, exacerbation, and death during centralized isolation and hospitalization. Prompt identification of comorbidities and complications in inpatients with COVID-19 can enhance the prevention of disease progression and death and improve the precision of risk predictions.
Keywords: COVID-19; centralized isolation and hospitalization; comorbidities; complications; systematic review.
Copyright © 2022 Chen, Peng, Wu, Pang, Yang, Zheng, Liu and Zhang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous