

Evaluation of the potential of Rejuveinix plus dexamethasone against sepsis
- PMID: 36052743
- PMCID: PMC9443789
- DOI: 10.2217/fmb-2022-0044
Evaluation of the potential of Rejuveinix plus dexamethasone against sepsis
Abstract
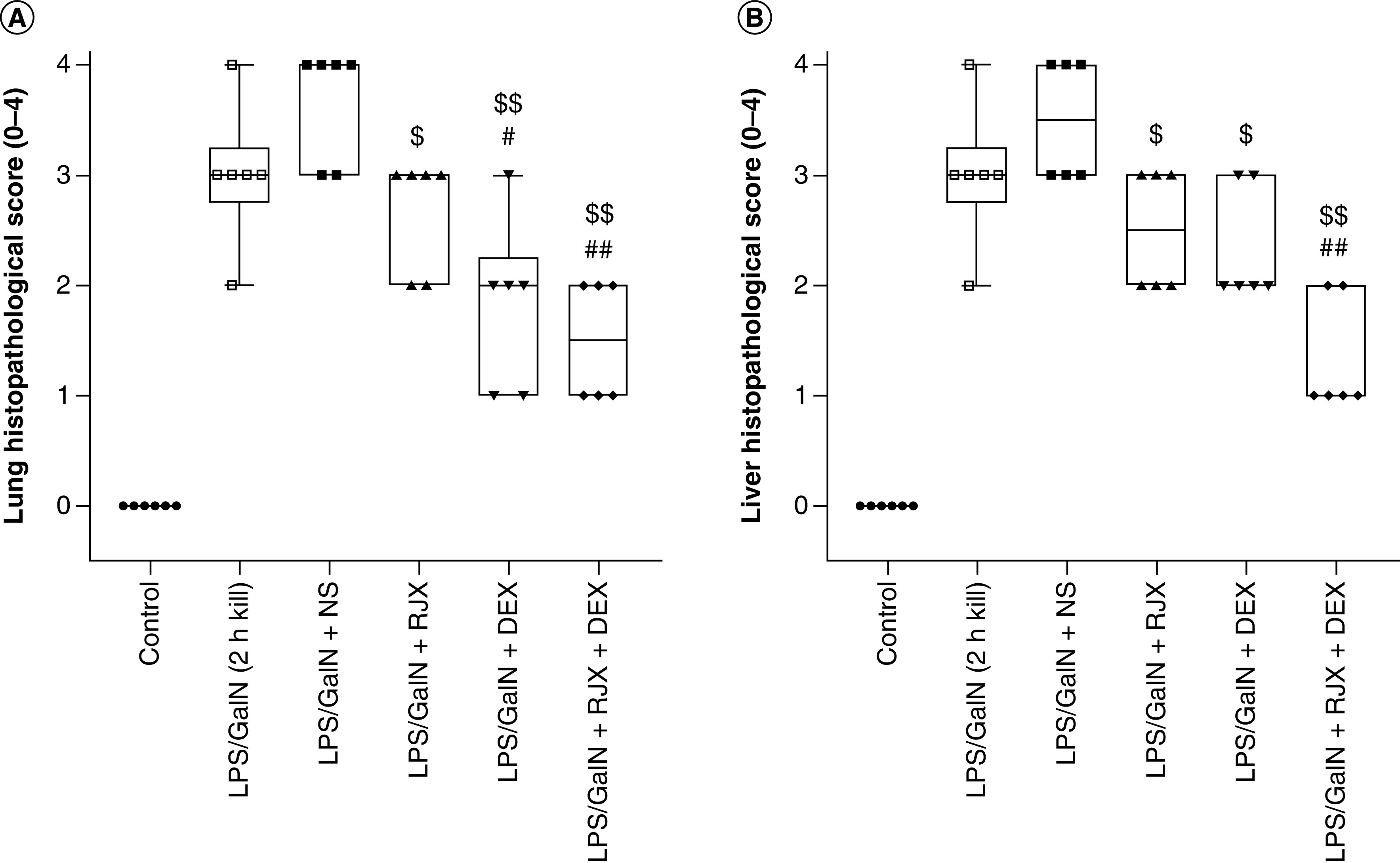
Aim: Our main objectives were to compare the effects of Rejuveinix (RJX), dexamethasone (DEX) and their combination on the severity of sepsis and survival outcome in an animal model of fatal sepsis. Methods: We used the LPS plus D-galactosamine mouse model of sepsis to compare the anti-inflammatory activities of RJX, dexamethasone and a combination of RJX plus DEX. Additionally, we examined the clinical feasibility and tolerability of combining RJX with DEX in COVID-19 patients in a clinical phase I study. Data were analyzed using standard methods. Results & conclusion: RJX exhibited potent anti-inflammatory activity in the murine sepsis model. The combination of RJX plus DEX was more effective than either agent alone, decreased the inflammatory cytokine responses and associated organ damage, and improved the survival outcome in mice. In the phase I clinical study, RJX plus DEX was well tolerated by COVID-19 patients.
Trial registration: ClinicalTrials.gov NCT03680105.
Keywords: COVID-19; LPS; RJX; inflammation; sepsis; vitamins.
Figures




References
-
- Rhodes A, Evans LE, Alhazzani W et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 43(3), 304–377 (2017). - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical