

Baseline Sex Differences in Pulmonary Arterial Hypertension Randomized Clinical Trials
- PMID: 36053665
- PMCID: PMC9819259
- DOI: 10.1513/AnnalsATS.202203-207OC
Baseline Sex Differences in Pulmonary Arterial Hypertension Randomized Clinical Trials
Abstract
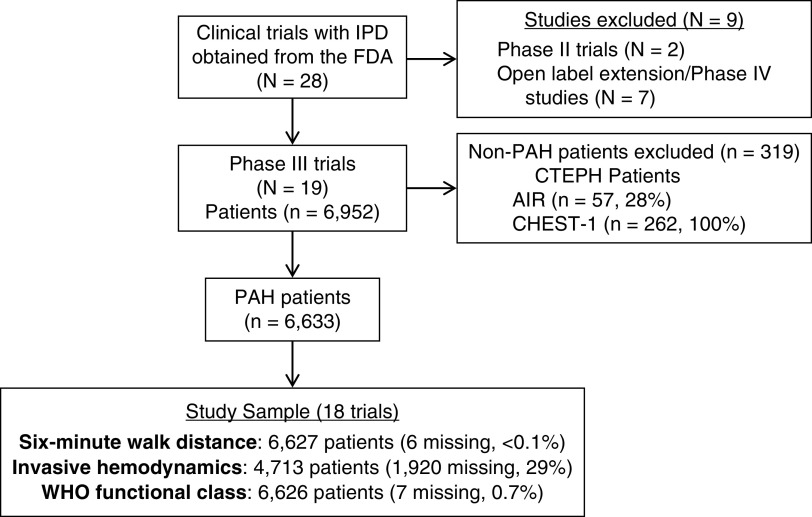
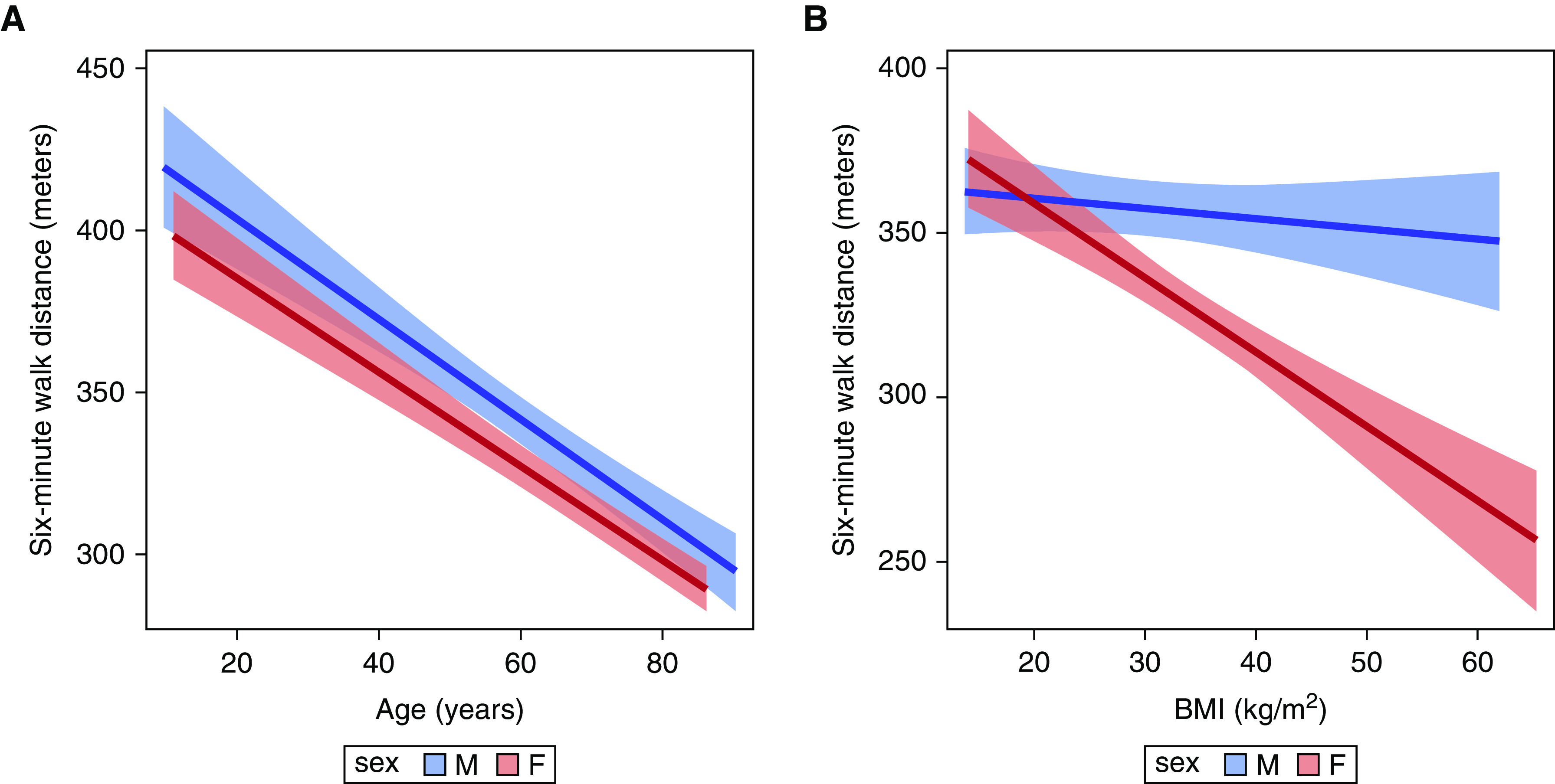
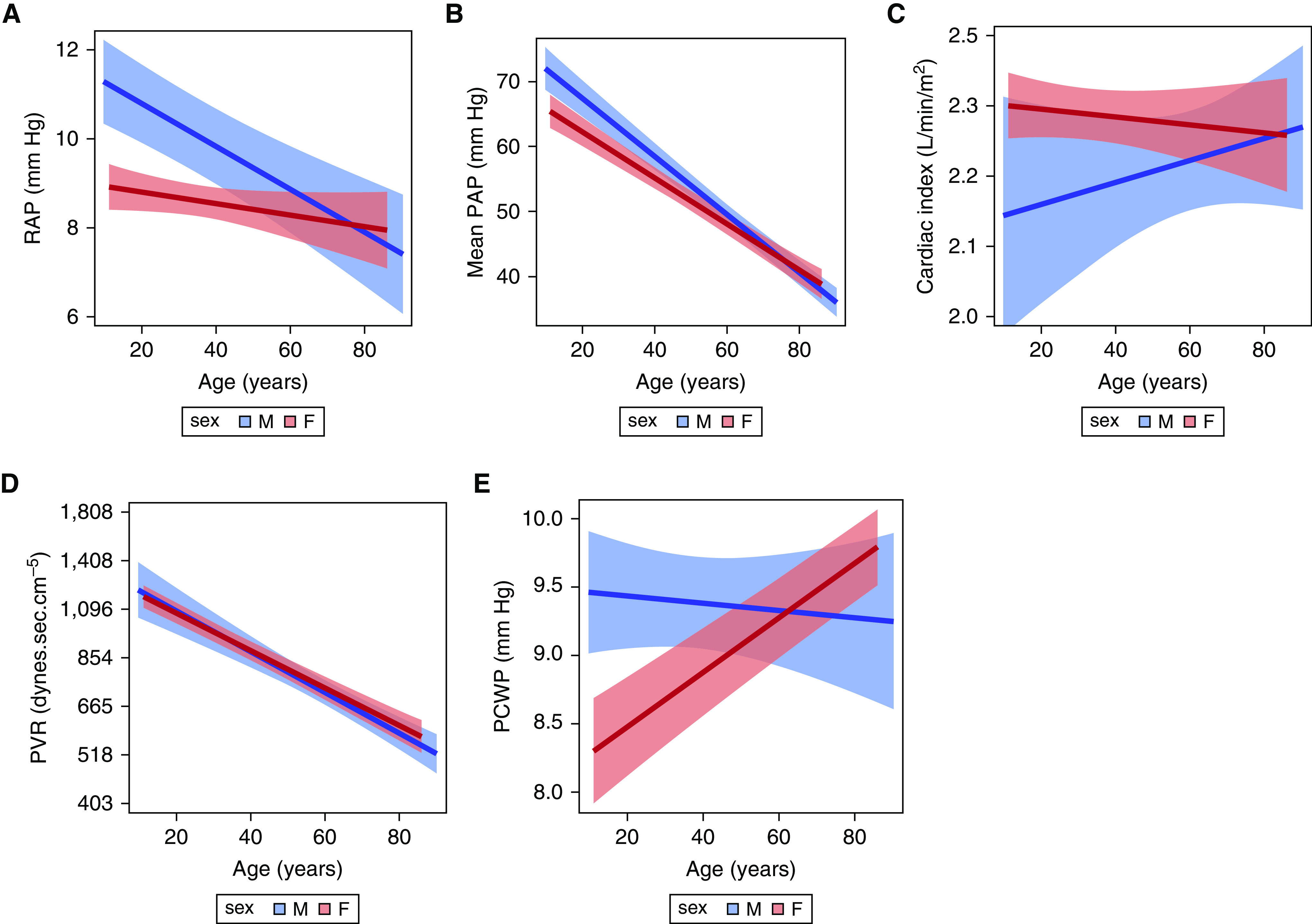
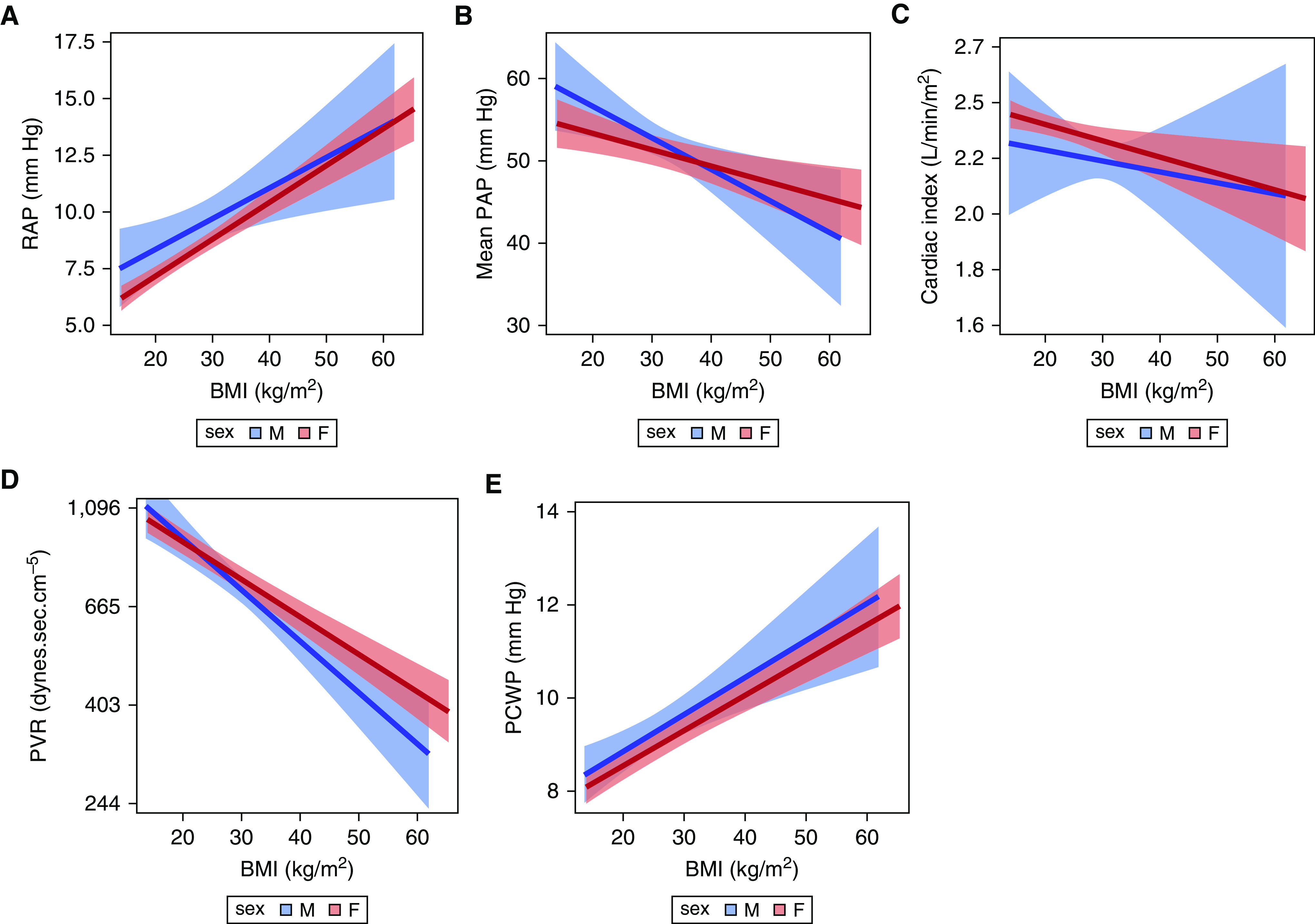
Rationale: Sex-based differences in pulmonary arterial hypertension (PAH) are known, but the contribution to disease measures is understudied. Objectives: We examined whether sex was associated with baseline 6-minute-walk distance (6MWD), hemodynamics, and functional class. Methods: We conducted a secondary analysis of participant-level data from randomized clinical trials of investigational PAH therapies conducted between 1998 and 2014 and provided by the U.S. Food and Drug Administration. Outcomes were modeled as a function of an interaction between sex and age or sex and body mass index (BMI), respectively, with generalized mixed modeling. Results: We included a total of 6,633 participants from 18 randomized clinical trials. A total of 5,197 (78%) were female, with a mean age of 49.1 years and a mean BMI of 27.0 kg/m2. Among 1,436 males, the mean age was 49.7 years, and the mean BMI was 26.4 kg/m2. The most common etiology of PAH was idiopathic. Females had shorter 6MWD. For every 1 kg/m2 increase in BMI for females, 6MWD decreased 2.3 (1.6-3.0) meters (P < 0.001), whereas 6MWD did not significantly change with BMI in males (0.31 m [-0.30 to 0.92]; P = 0.32). Females had lower right atrial pressure (RAP) and mean pulmonary artery pressure, and higher cardiac index than males (all P < 0.03). Age significantly modified the sex by RAP and mean pulmonary artery pressure relationships. For every 10-year increase in age, RAP was lower in males (0.5 mm Hg [0.3-0.7]; P < 0.001), but not in females (0.13 [-0.03 to 0.28]; P = 0.10). There was a significant decrease in pulmonary vascular resistance (PVR) with increasing age regardless of sex (P < 0.001). For every 1 kg/m2 increase in BMI, there was a 3% decrease in PVR for males (P < 0.001), compared with a 2% decrease in PVR in females (P < 0.001). Conclusions: Sexual dimorphism in subjects enrolled in clinical trials extends to 6MWD and hemodynamics; these relationships are modified by age and BMI. Sex, age, and body size should be considered in the evaluation and interpretation of surrogate outcomes in PAH.
Keywords: body mass index; pulmonary arterial hypertension; sex; sexual dimorphism.
Figures
References
-
- Boucly A, Weatherald J, Savale L, Jais X, Cottin V, Prevot G, et al. Risk assessment, prognosis and guideline implementation in pulmonary arterial hypertension. Eur Respir J . 2017;50:1700889. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
