

Immune thrombocytopenia and pregnancy: an exposed/nonexposed cohort study
- PMID: 36054922
- PMCID: PMC10644036
- DOI: 10.1182/blood.2022017277
Immune thrombocytopenia and pregnancy: an exposed/nonexposed cohort study
Abstract
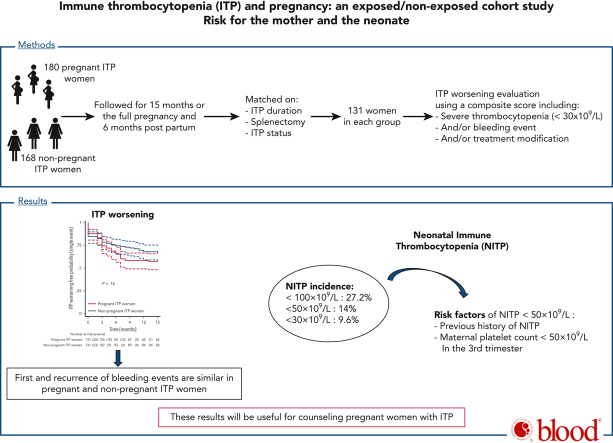
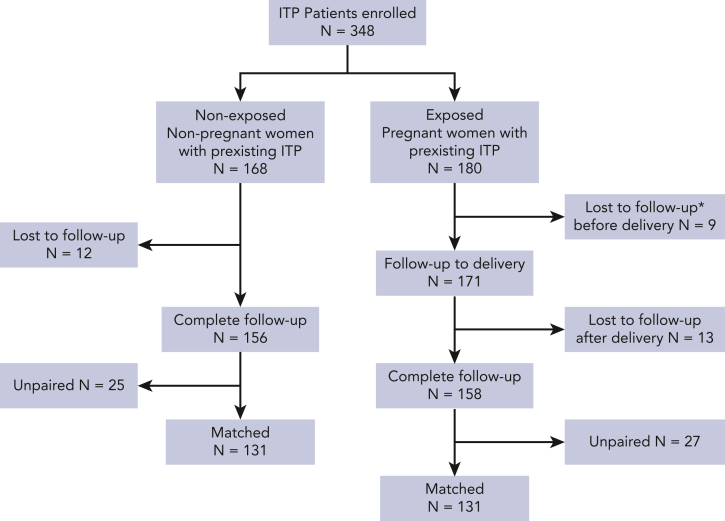
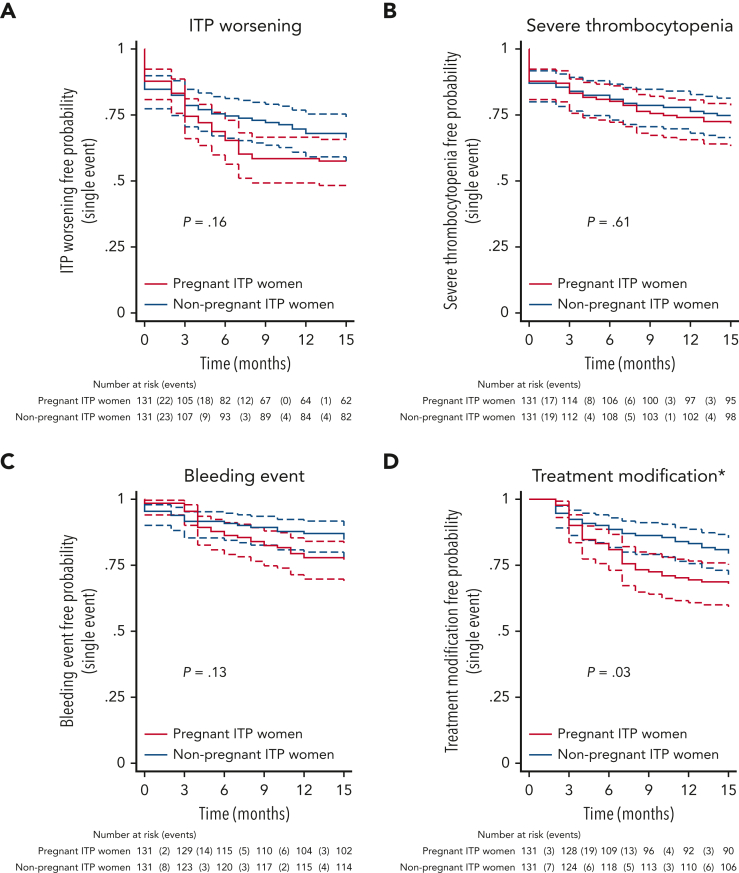
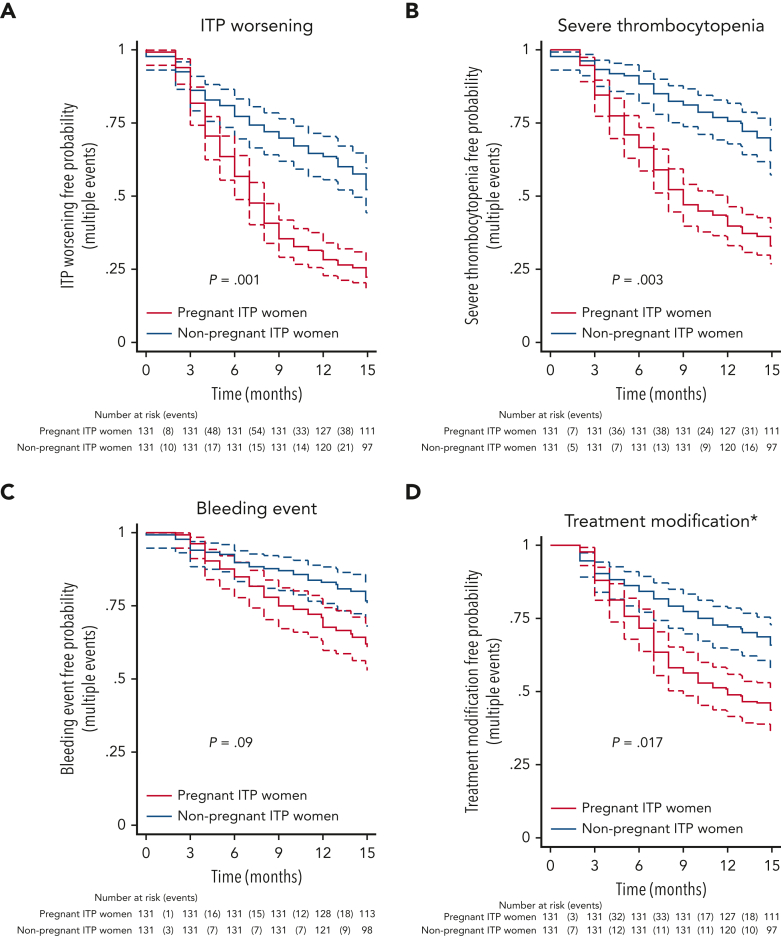
The risk of immune thrombocytopenia (ITP) worsening during pregnancy and neonatal ITP (NITP) have never been prospectively studied. We included 180 pregnant and 168 nonpregnant women with ITP in a prospective, multicenter, observational cohort study. A total of 131 pregnant women with ITP were matched to 131 nonpregnant women with ITP by history of splenectomy, ITP status (no response, response, complete response), and duration. Groups were followed for 15 months. The primary outcome was the first occurrence of ITP worsening defined by a composite end point including bleeding events and/or severe thrombocytopenia (<30 × 109/L) and/or ITP treatment modification. We also studied the recurrence of ITP worsening and the incidence of NITP and risk factors. The first occurrence of ITP worsening did not differ between pregnant and nonpregnant women with ITP (53.4 per 100 person-years [95% confidence interval {CI}, 40.8-69.9] vs 37.1 [95% CI, 27.5-50.0]; hazard ratio {HR}, 1.35 [95% CI, 0.89-2.03], P = .16). Pregnant women with ITP were more likely to have recurrence of severe thrombocytopenia and treatment modification (HR, 2.71 [95% CI, 1.41-5.23], P = .003; HR, 2.01 [95% CI, 1.14-3.57], P = .017, respectively). However, recurrence of severe bleeding events was not different between groups (P = .4). Nineteen (14%) neonates showed NITP <50 × 109/L. By multivariable analysis, NITP was associated with a previous offspring with NITP and maternal platelet count <50 × 109/L within 3 months before delivery (adjusted odds ratio, 5.55 [95% CI, 1.72-17.89], P = .004 and 4.07 [95% CI, 1.41-11.73], P = .009). To conclude, women with ITP do not increase their risk of severe bleeding during pregnancy. NITP is associated with NITP history and the severity of maternal ITP during pregnancy. These results will be useful for counseling women with ITP.
© 2023 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: B.G. serves as expert for AMGEN, Novartis, Grifols, Sobi, and Borhinger. M. Mahevas received funds for research from GSK, and received fees from LFB. M. Michel received consultancy fees from Amgen, Novartis, and Argenx. D.G. received consultancy fees from Novartis and Shire Takeda. The remaining authors declare no competing financial interests.
Figures
Comment in
-
What to expect when an ITP patient is expecting.Blood. 2023 Jan 5;141(1):3-4. doi: 10.1182/blood.2022018082. Blood. 2023. PMID: 36602822 No abstract available.
References
-
- Webert KE, Mittal R, Sigouin C, Heddle NM, Kelton JG. A retrospective 11-year analysis of obstetric patients with idiopathic thrombocytopenic purpura. Blood. 2003;102(13):4306–4311. - PubMed
-
- Fujita A, Sakai R, Matsuura S, et al. A retrospective analysis of obstetric patients with idiopathic thrombocytopenic purpura: a single center study. Int J Hematol. 2010;92(3):463–467. - PubMed
-
- Loustau V, Debouverie O, Canoui-Poitrine F, et al. Effect of pregnancy on the course of immune thrombocytopenia: a retrospective study of 118 pregnancies in 82 women. Br J Haematol. 2014;166(6):929–935. - PubMed
-
- Ali R, Ozkalemkaş F, Ozçelik T, et al. Idiopathic thrombocytopenic purpura in pregnancy: a single institutional experience with maternal and neonatal outcomes. Ann Hematol. 2003;82(6):348–352. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
