

Adverse Effects of Excessive Zinc Intake in Infants and Children Aged 0-3 Years: A Systematic Review and Meta-Analysis
- PMID: 36055780
- PMCID: PMC9776731
- DOI: 10.1093/advances/nmac088
Adverse Effects of Excessive Zinc Intake in Infants and Children Aged 0-3 Years: A Systematic Review and Meta-Analysis
Abstract
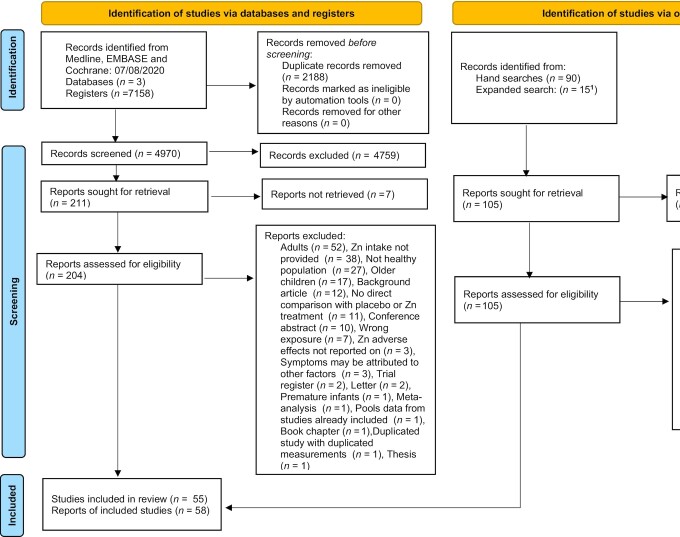
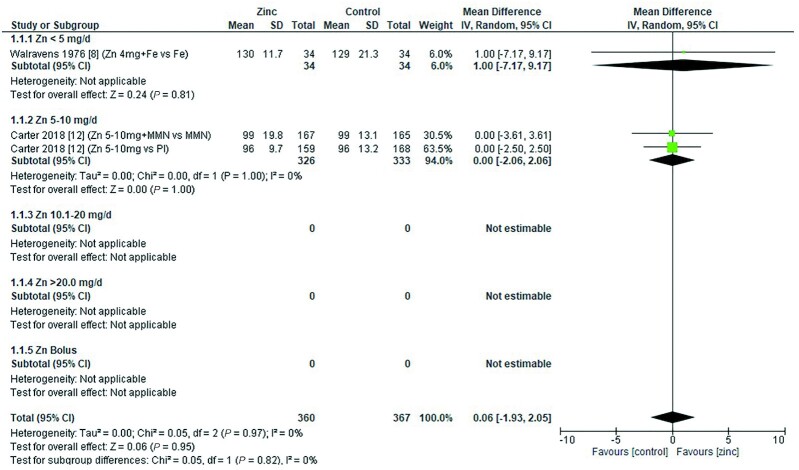
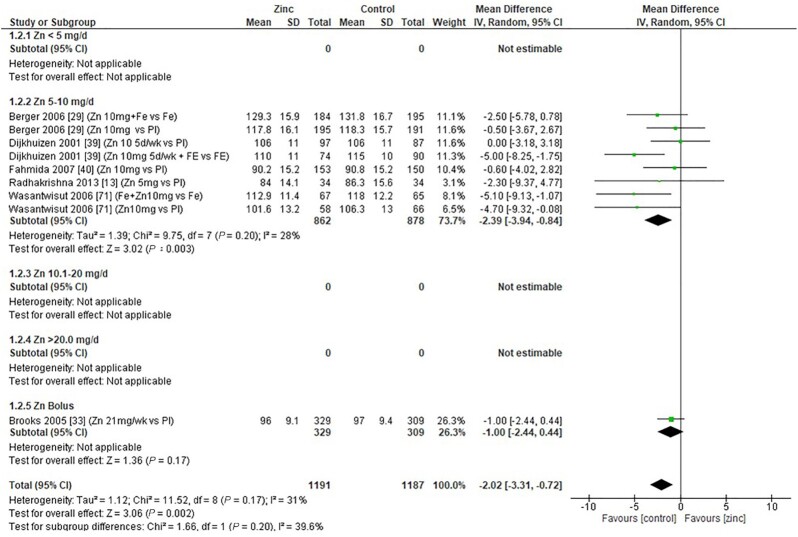
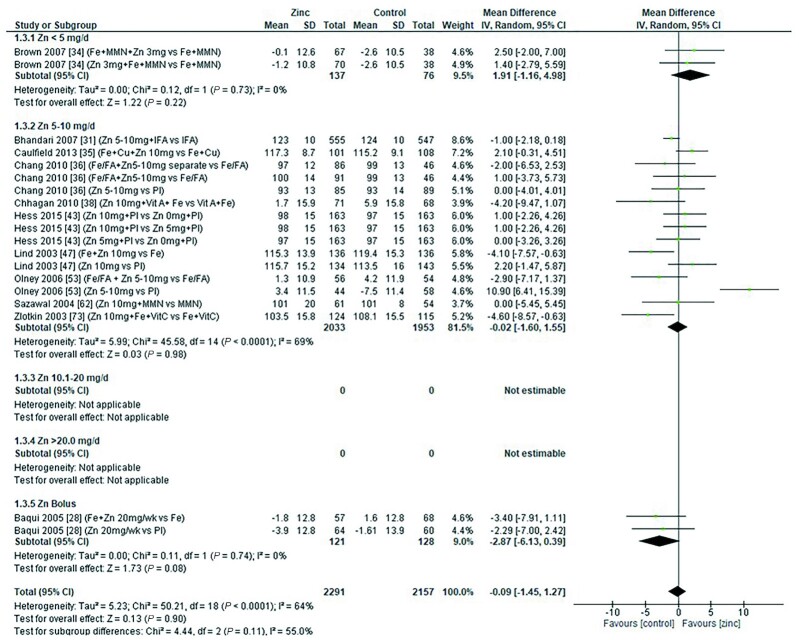
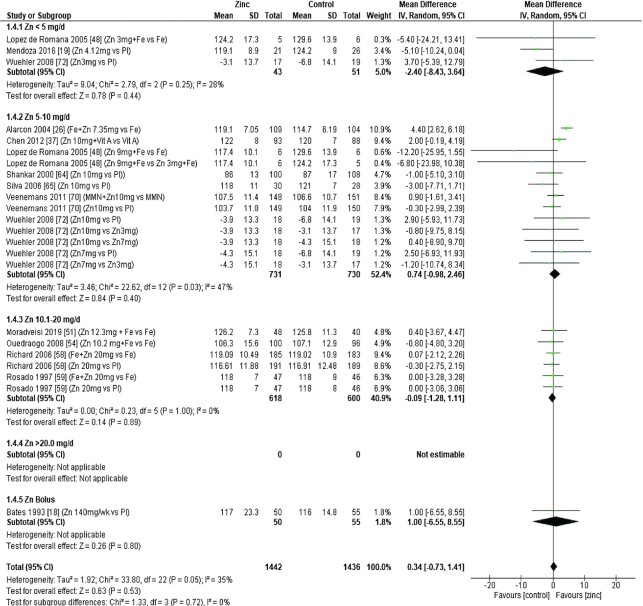
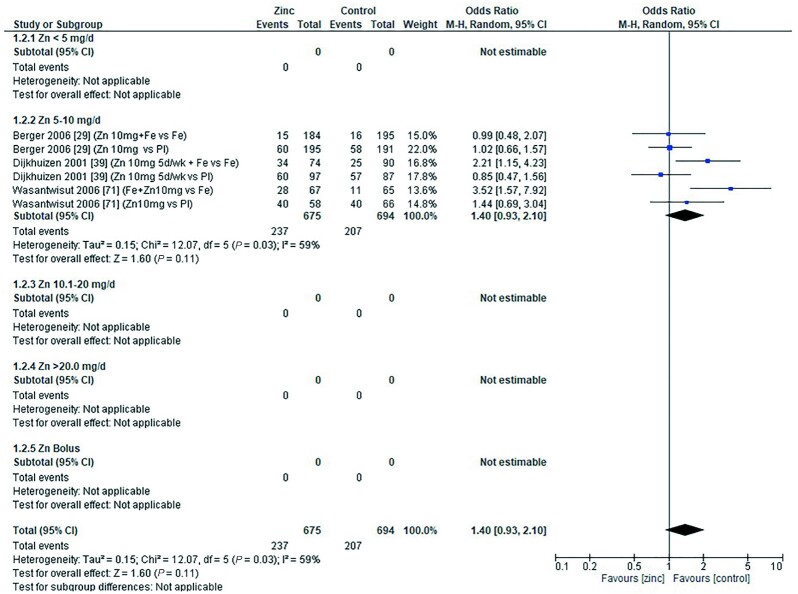
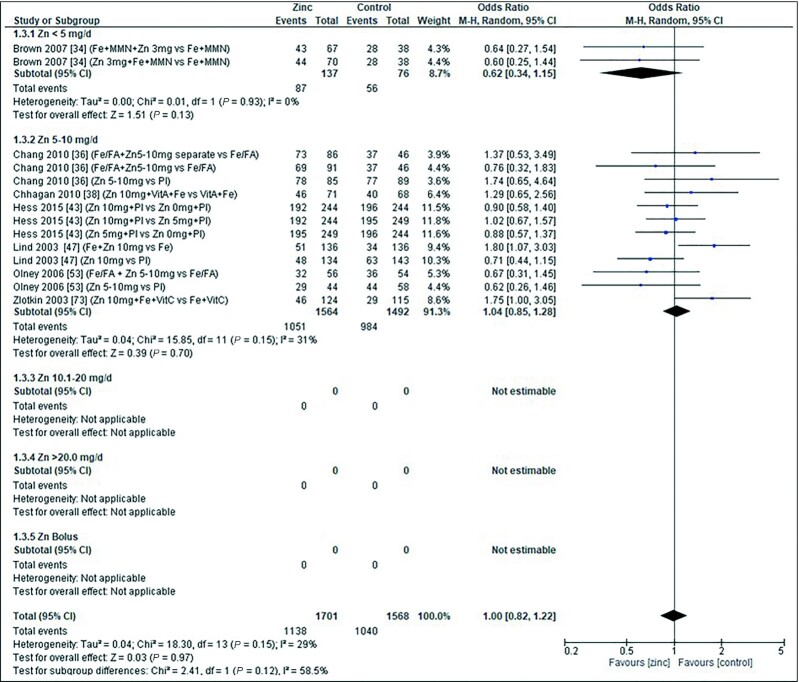
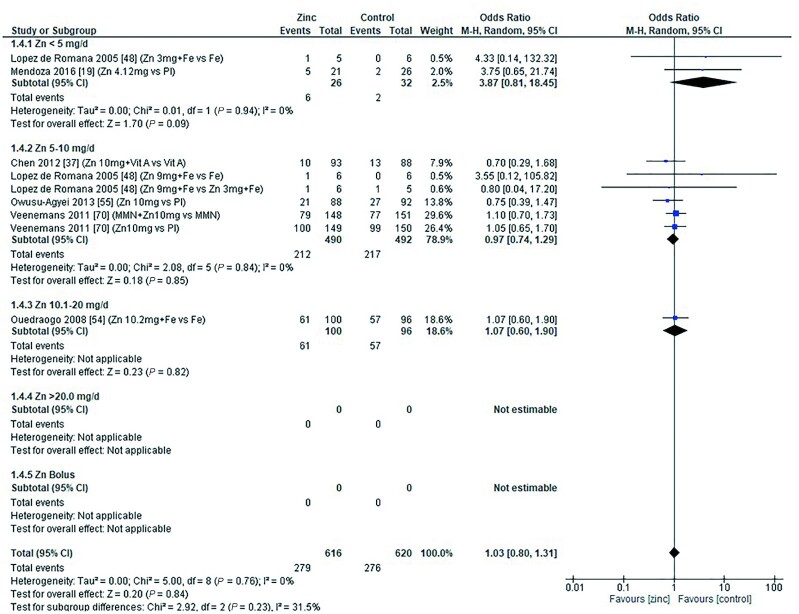
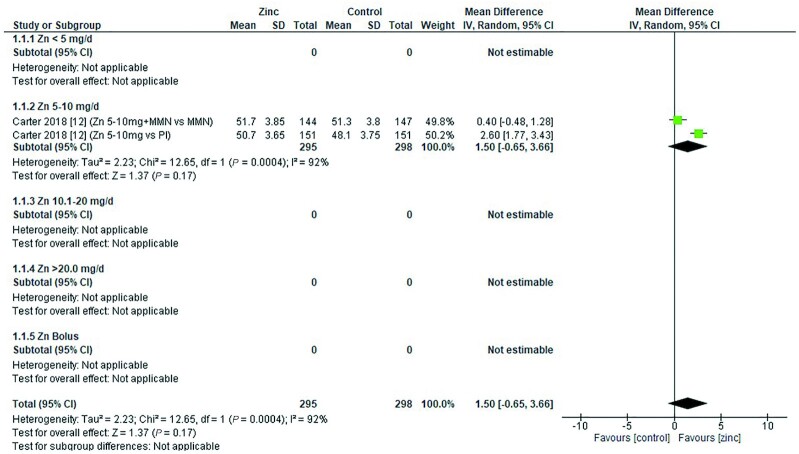
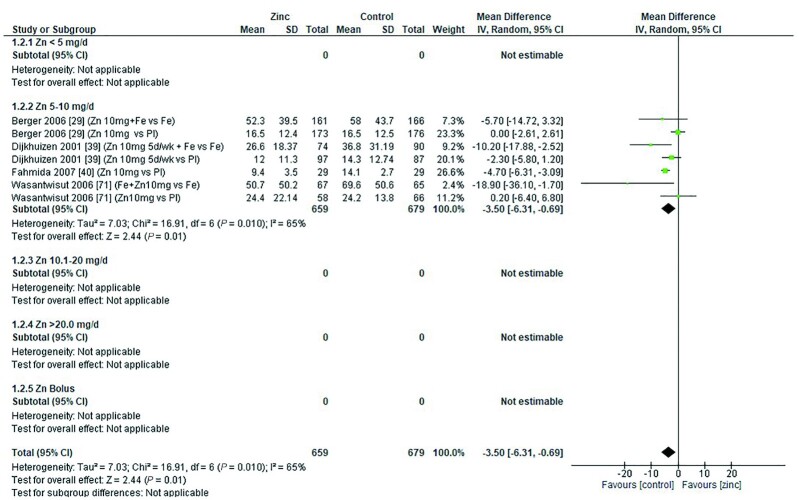
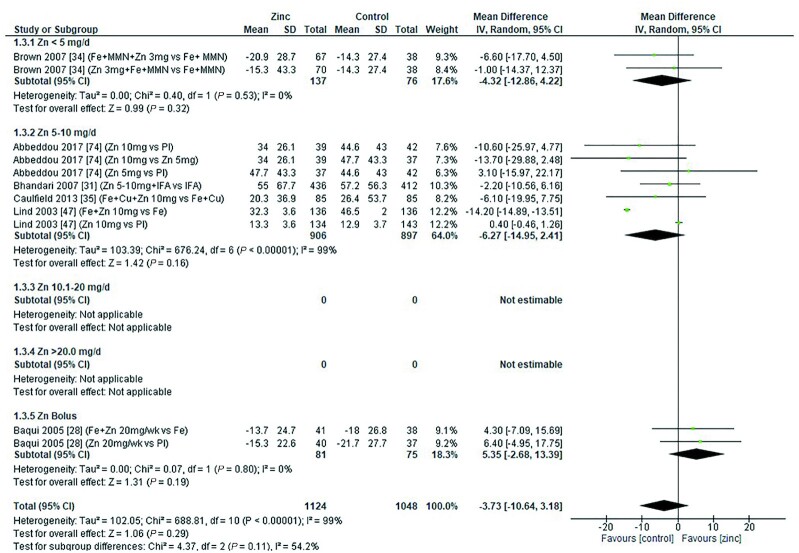
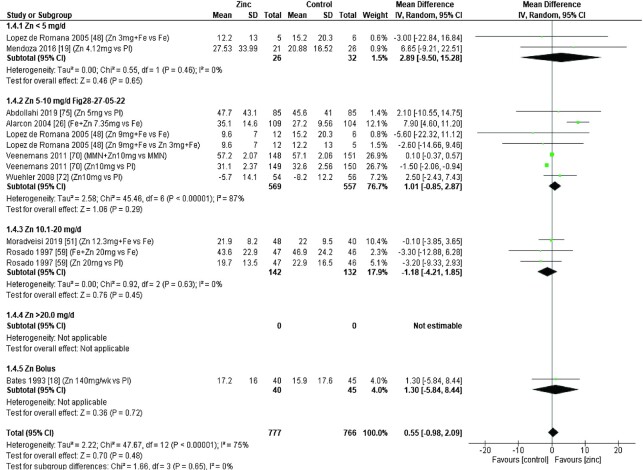
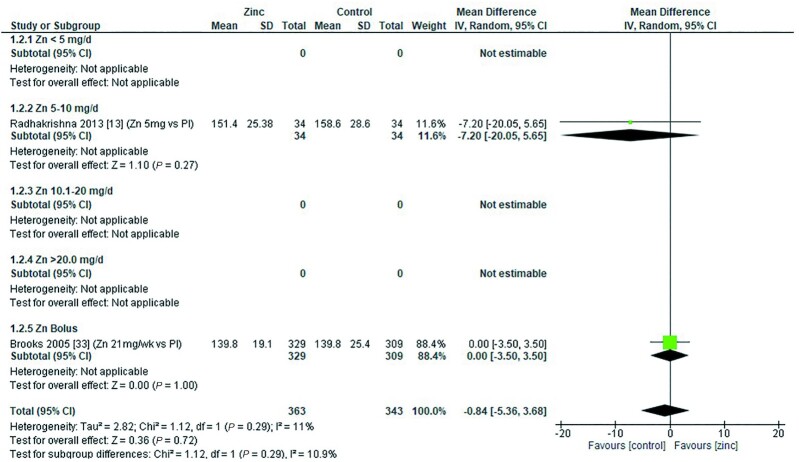
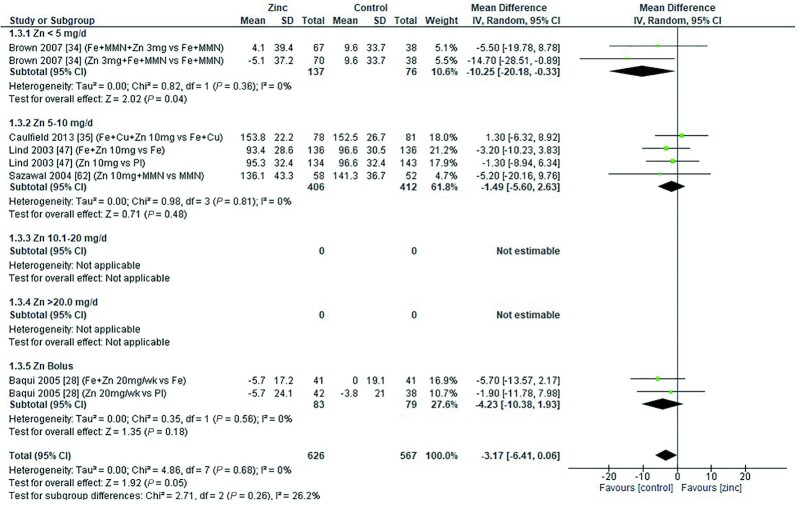
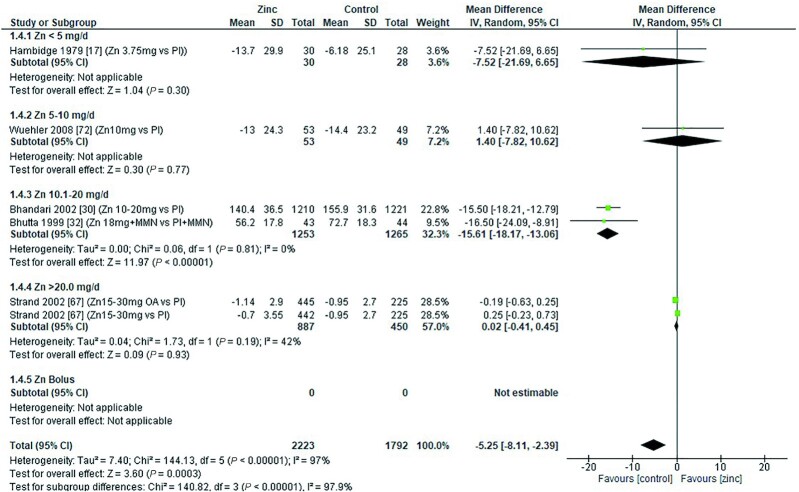
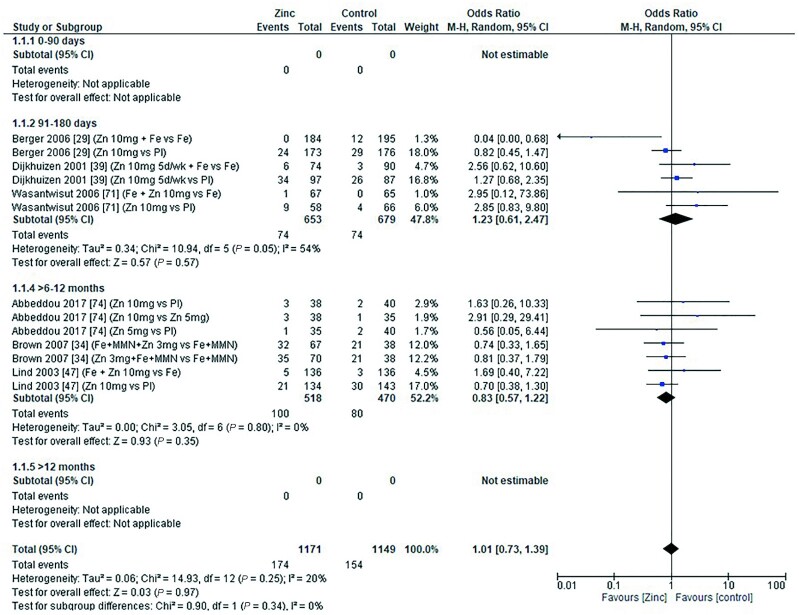
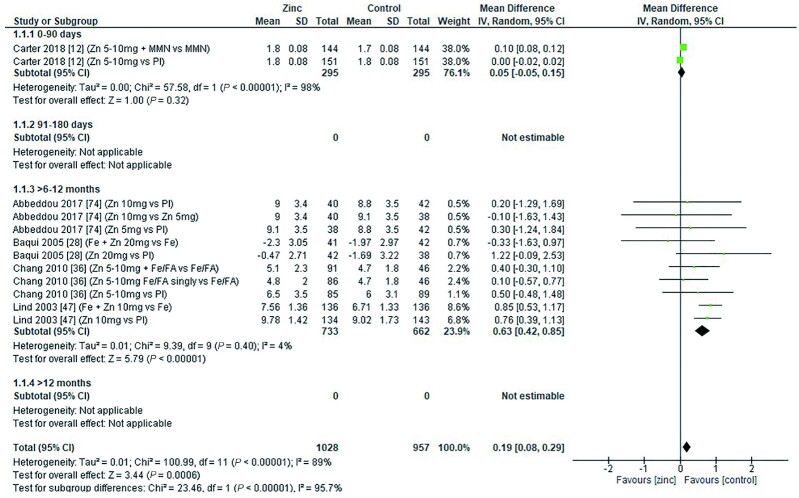
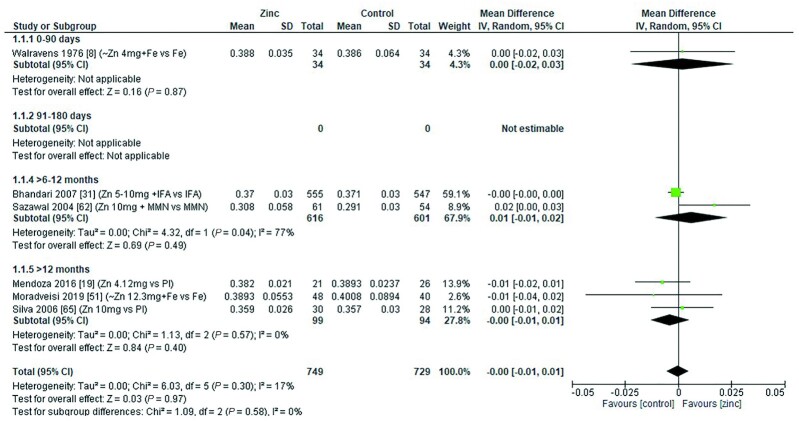
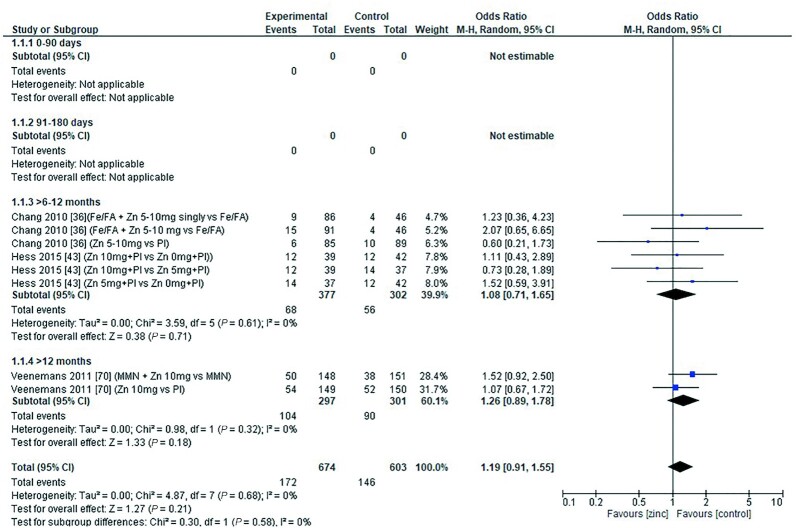
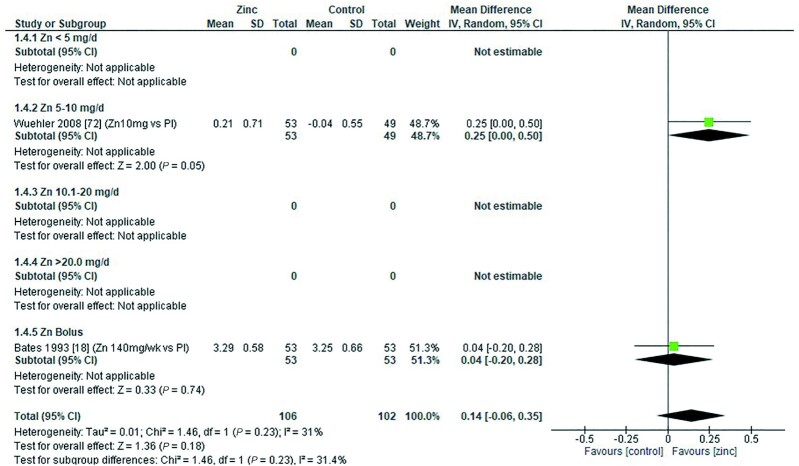
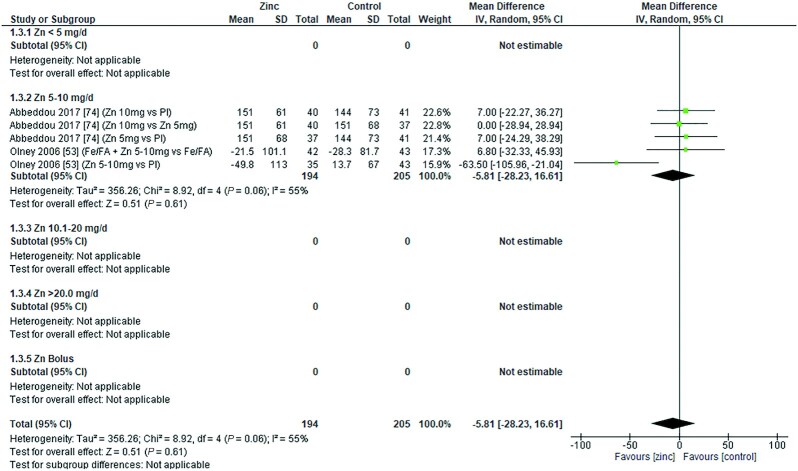
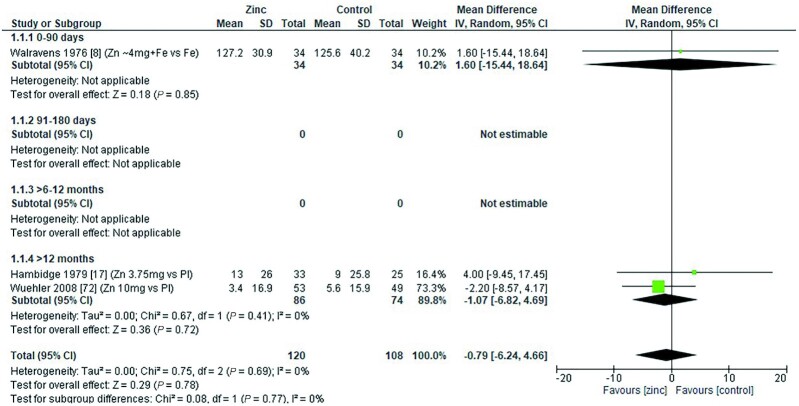
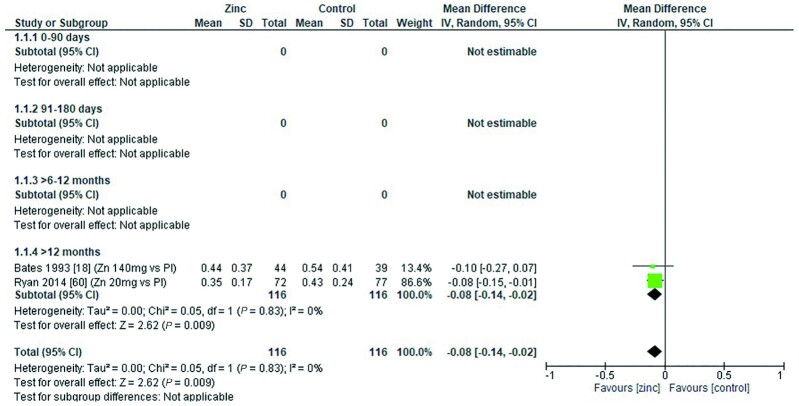
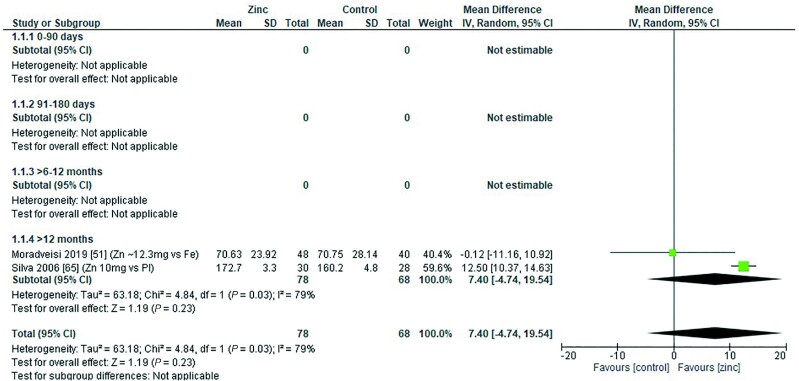
Zinc supplementation reduces morbidity, but evidence suggests that excessive intakes can have negative health consequences. Current guidelines of upper limits (ULs) of zinc intake for young children are extrapolated from adult data. This systematic review (PROSPERO; registration no. CRD42020215187) aimed to determine the levels of zinc intake at which adverse effects are observed in young children. Studies reporting potential adverse effects of zinc intake in children aged 0-3 y were identified (from inception to August 2020) in MEDLINE, Embase, and the Cochrane Library, with no limits on study design. Adverse clinical and physical effects of zinc intake were synthesized narratively, and meta-analyses of biochemical outcomes were conducted. Random effects models were used to generate forest plots to examine the evidence by age category, dose, dose duration, chemical formula of zinc, and zinc compared with placebo. The Joanna Briggs Institute Critical Appraisal Checklist, Cochrane Risk of Bias 2, and Grading of Recommendations Assessment, Development, and Evaluation (GRADE) guideline were employed to assess risk of bias and to appraise the certainty of evidence. Fifty-eight studies assessed possible adverse effects of zinc doses ranging from 3 to 70 mg/d. Data from 39 studies contributed to meta-analyses. Zinc supplementation had an adverse effect on serum ferritin, plasma/serum copper concentration, serum transferrin receptor, hemoglobin, hematocrit, and the odds of anemia in ≥1 of the subgroups investigated. Lactulose:mannitol ratio was improved with zinc supplementation, and no significant effect was observed on C-reactive protein, erythrocyte superoxide dismutase, zinc protoporphyrin, blood cholesterol, and iron deficiency anemia. The certainty of the evidence, as assessed using GRADE, was very low to moderate. Although possible adverse effects of zinc supplementation were observed in some subgroups, it is unclear whether these findings are clinically important. The synthesized data can be used to undertake a dose-response analysis to update current guidelines of ULs of zinc intake for young children.
Keywords: children; dietary requirements; meta-analysis; systematic review; upper limits; zinc.
© The Author(s) 2022. Published by Oxford University Press on behalf of the American Society for Nutrition.
Figures

References
-
- World Health Organization/Food and Agriculture Organization of the United Nations . Vitamin and mineral requirements in human nutrition, 2nd ed[Internet]. Geneva, Siwtzerland:World Health Organization; 2004 [cited August 30, 2022]. Available from: http://apps.who.int/iris/bitstream/handle/10665/42716/9241546123.pdf;jse...
-
- FAO/WHO (Food and Agricultural Organization of the UN/World Health Organization) Expert Consultation . Application of risk analysis to food standards issues. Recommendations to the Codex Alimentarius Commission (Alinorm 95/9, Appendix 5). Geneva: WHO; 1995.
-
- European Food Safety Authority (EFSA) . Tolerable upper intake level on vitamins and minerals. [Internet]. 2006; [cited August 30, 2022]. Available from: https://www.efsa.europa.eu/sites/default/files/efsa_rep/blobserver_asset...
-
- King JC, Shames DM, Woodhouse LR. Zinc homeostasis in humans. J Nutr. 2000;130(5S Suppl):1360S–6S. - PubMed
-
- Fosmire GJ. Zinc toxicity. Am J Clin Nutr. 1990;51(2):225–27. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
