

Influence of Cancer on COVID-19 Incidence, Outcomes, and Vaccine Effectiveness: A Prospective Cohort Study of U.S. Veterans
- PMID: 36055952
- PMCID: PMC9353607
- DOI: 10.1053/j.seminoncol.2022.07.005
Influence of Cancer on COVID-19 Incidence, Outcomes, and Vaccine Effectiveness: A Prospective Cohort Study of U.S. Veterans
Abstract
Purpose: Coronavirus disease 2019 (COVID-19) has been a constant health threat since its emergence. Amongst risk factors proposed, a diagnosis of cancer has been worrisome. We report the impact of cancer and other risk factors in US Veterans receiving care at Veterans Administration (VA) Hospitals, their adjusted odds ratio (aOR) for infection and death, and report on the impact of vaccines on the incidence and severity of COVID-19 infections in Veterans without/with cancer.
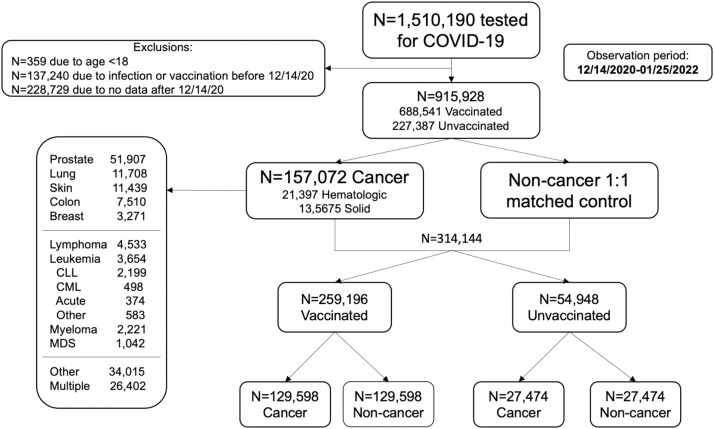
Methods: We conducted a cohort study of US Veterans without/with cancer by mining VA COVID-19 Shared Data Resource (CSDR) data using the VA Informatics and Computing Infrastructure (VINCI). Our observation period includes index dates from 14DEC2020 to 25JAN2022, encompassing both the delta and omicron waves in the US.
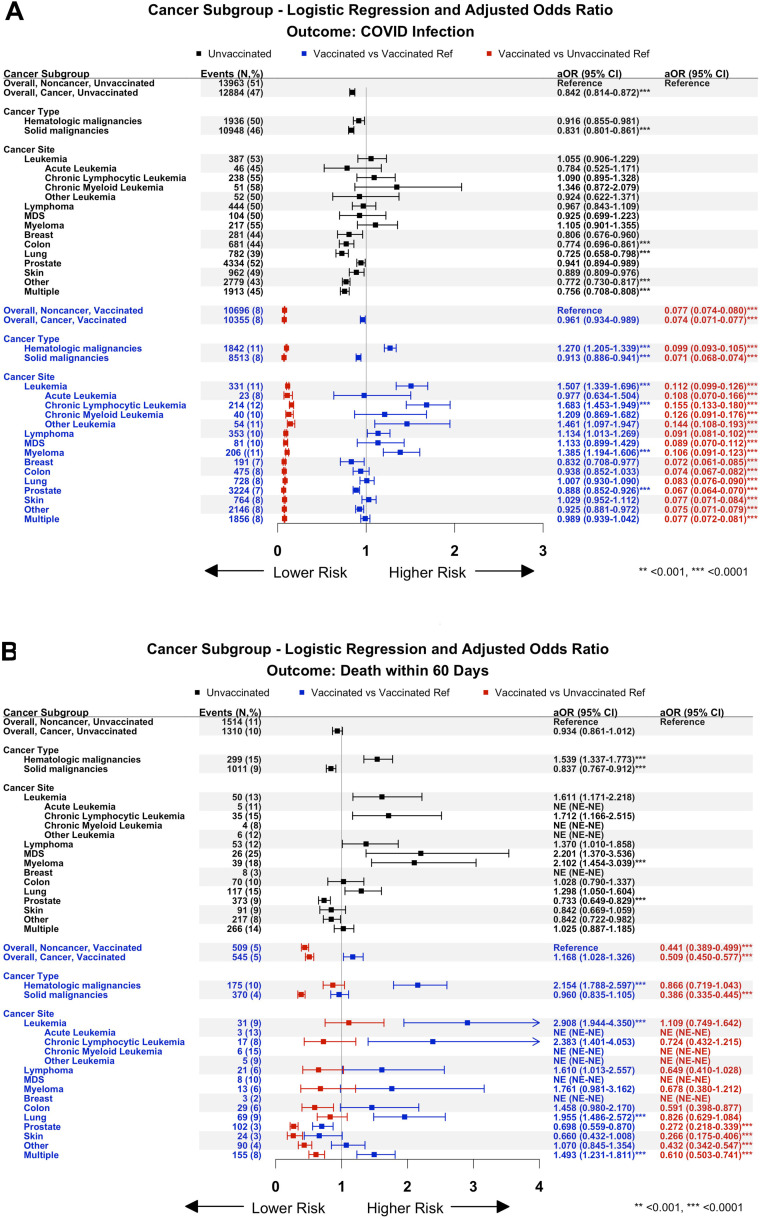
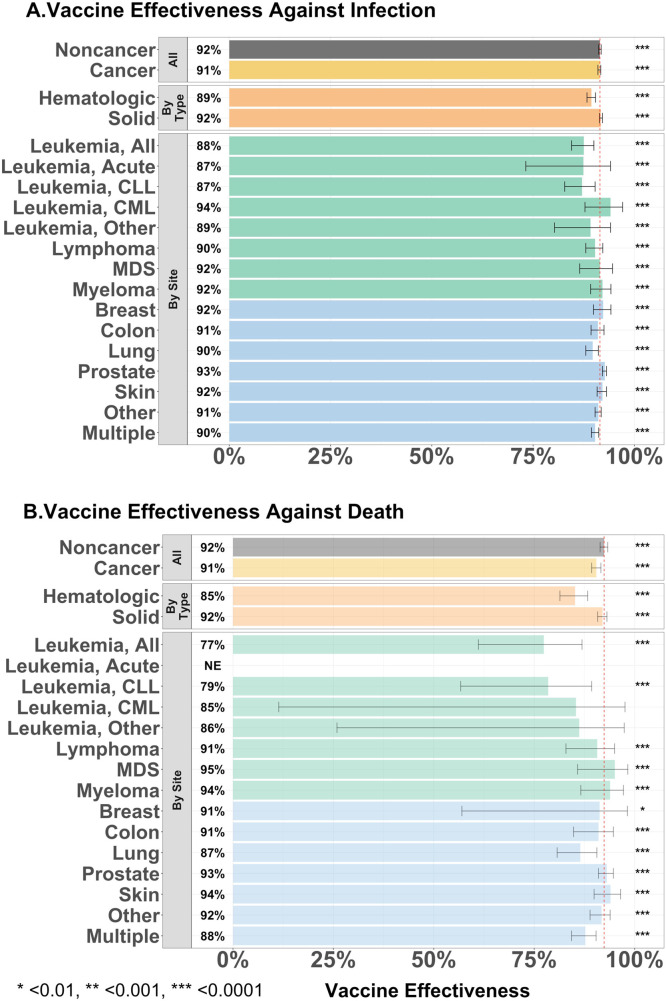
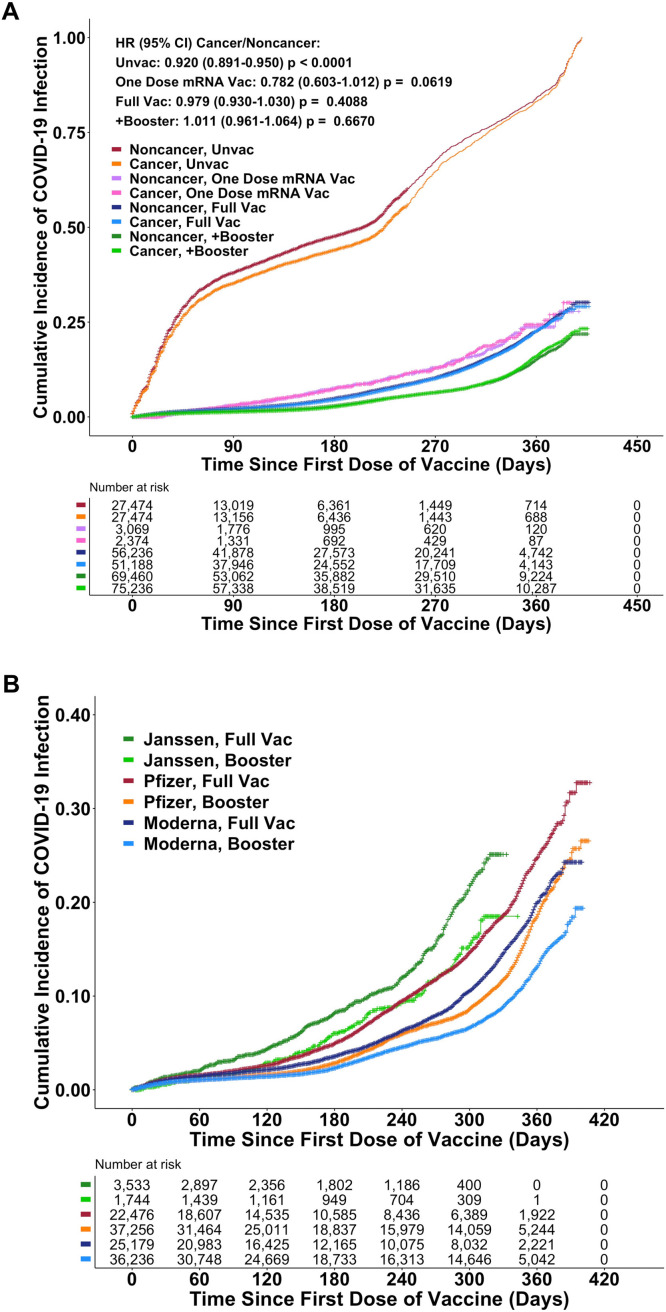
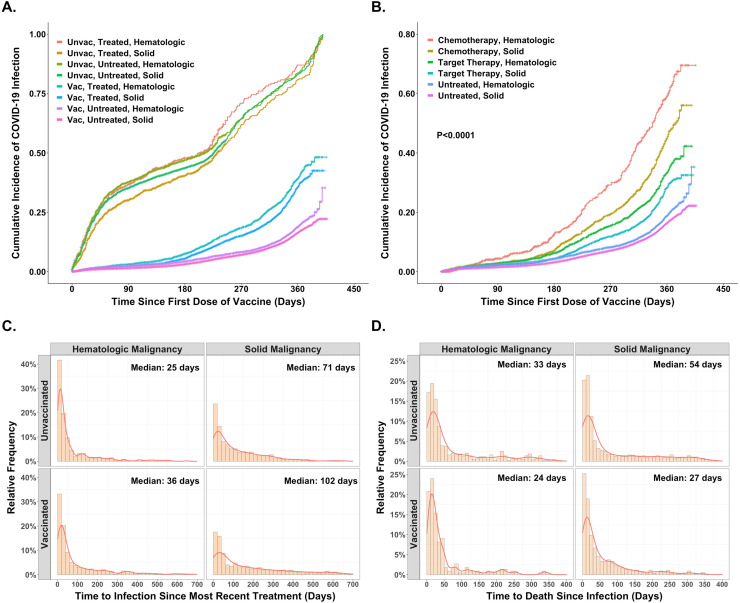
Results: We identified 915,928 Veterans, 24% of whom were African Americans who had undergone COVID testing-688,541 were and 227,387 were not vaccinated. 157,072 had a cancer diagnosis in the preceding two years. Age emerged as the major risk factor, with gender, BMI, and (Elixhauser) comorbidity contributing less. Among veterans with solid tumors other than lung cancer, risks of infection and death within 60 days were comparable to Veterans without cancer. However, those with hematologic malignancies fared worse. Vaccination was highly effective across all cancer cohorts; the respective rates of infection and death after infection were 8% and 5% among the vaccinated compared to 47% and 10% in the unvaccinated. Amongst vaccinated, increased risk of infection was noted in both, Veterans with hematologic malignancy treated with chemotherapy (HR, 2.993, P < 0.0001) or targeted therapies (HR, 1.781, P < 0.0001), and in solid tumors treated with either chemotherapy (HR 2.328, 95%CI 2.075-2.611, P < 0.0001) or targeted therapies (HR 1.328, P < 0.0001) when compared to those not on treatment.
Conclusions: Risk for COVID-19 infection and death from infection vary based on cancer type and therapies administered. Importantly and encouragingly, the duration of protection from infection following vaccination in Veterans with a diagnosis of cancer was remarkably like those without a cancer diagnosis. Veterans with hematologic malignancies are especially vulnerable, with lower vaccine effectiveness (VE).
Keywords: Cancer; Chemotherapy; Covid-19 vaccine effectiveness; Hematologic malignancies; Immunotherapy; Solid tumors.
Copyright © 2022 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of Interest None
Figures
References
-
- WHO. Weekly epidemiological update on COVID-19 - 27 April 2022. Available from: https://www.who.int/publications/m/item/weekly-epidemiological-update-on...—27-april-2022.
-
- Gao YD, Ding M, Dong X, et al. Risk factors for severe and critically ill COVID-19 patients: a review. Allergy. 2021;76(2):428–455. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
