

The trend of disruption in the functional brain network topology of Alzheimer's disease
- PMID: 36056059
- PMCID: PMC9440254
- DOI: 10.1038/s41598-022-18987-y
The trend of disruption in the functional brain network topology of Alzheimer's disease
Abstract
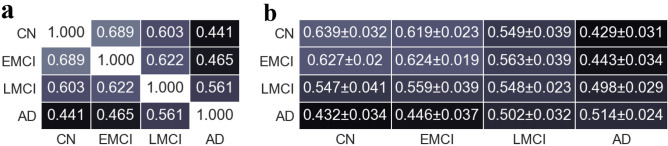
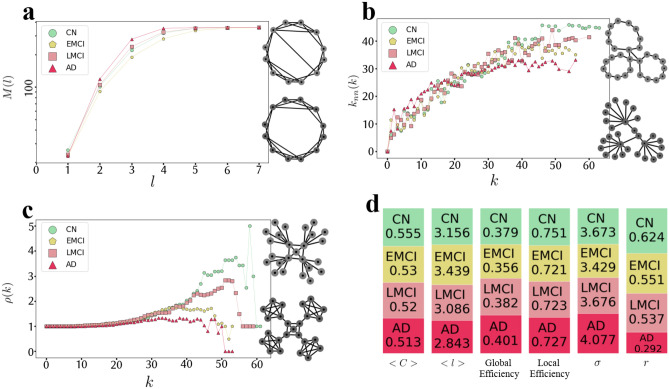
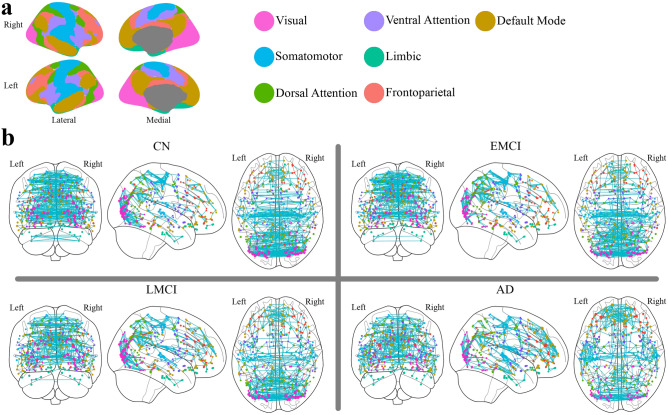
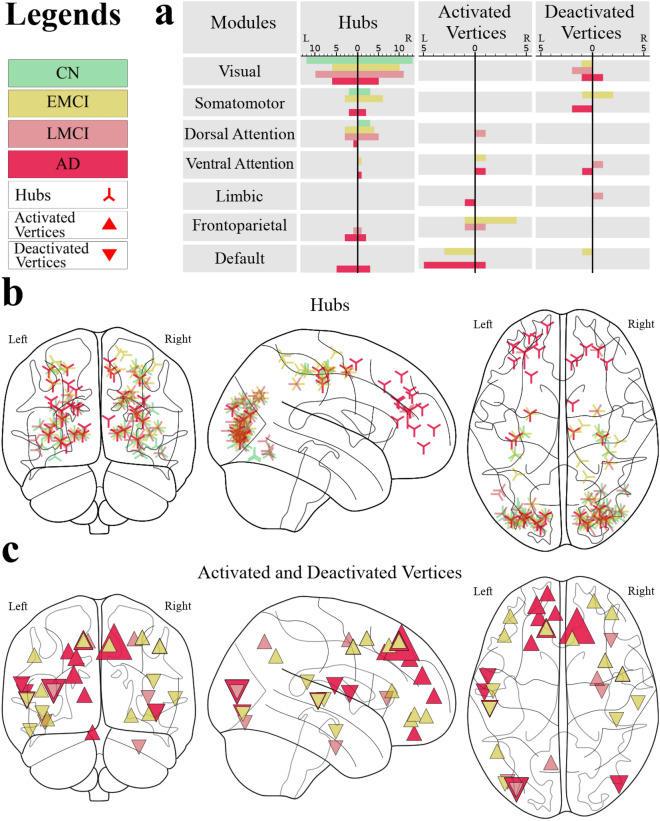
Alzheimer's disease (AD) is a progressive disorder associated with cognitive dysfunction that alters the brain's functional connectivity. Assessing these alterations has become a topic of increasing interest. However, a few studies have examined different stages of AD from a complex network perspective that cover different topological scales. This study used resting state fMRI data to analyze the trend of functional connectivity alterations from a cognitively normal (CN) state through early and late mild cognitive impairment (EMCI and LMCI) and to Alzheimer's disease. The analyses had been done at the local (hubs and activated links and areas), meso (clustering, assortativity, and rich-club), and global (small-world, small-worldness, and efficiency) topological scales. The results showed that the trends of changes in the topological architecture of the functional brain network were not entirely proportional to the AD progression. There were network characteristics that have changed non-linearly regarding the disease progression, especially at the earliest stage of the disease, i.e., EMCI. Further, it has been indicated that the diseased groups engaged somatomotor, frontoparietal, and default mode modules compared to the CN group. The diseased groups also shifted the functional network towards more random architecture. In the end, the methods introduced in this paper enable us to gain an extensive understanding of the pathological changes of the AD process.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- 2020 alzheimer’s disease facts and figures. Alzheimer’s & Dementia16, 391–460. 10.1002/alz.12068. https://alz-journals.onlinelibrary.wiley.com/doi/pdf/10.1002/alz.12068. - DOI - PubMed
-
- Organization, W. H. Global Tuberculosis Report 2019. Global tuberculosis control (World Health Organization, 2019).
