

Spike-based adenovirus vectored COVID-19 vaccine does not aggravate heart damage after ischemic injury in mice
- PMID: 36056135
- PMCID: PMC9439278
- DOI: 10.1038/s42003-022-03875-y
Spike-based adenovirus vectored COVID-19 vaccine does not aggravate heart damage after ischemic injury in mice
Abstract
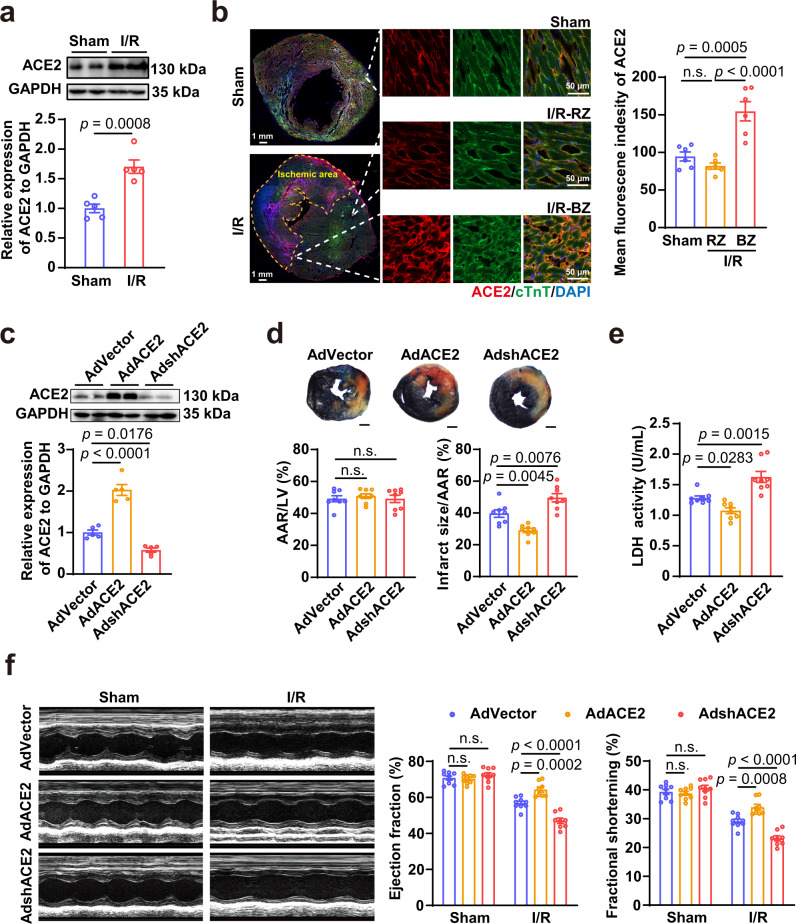
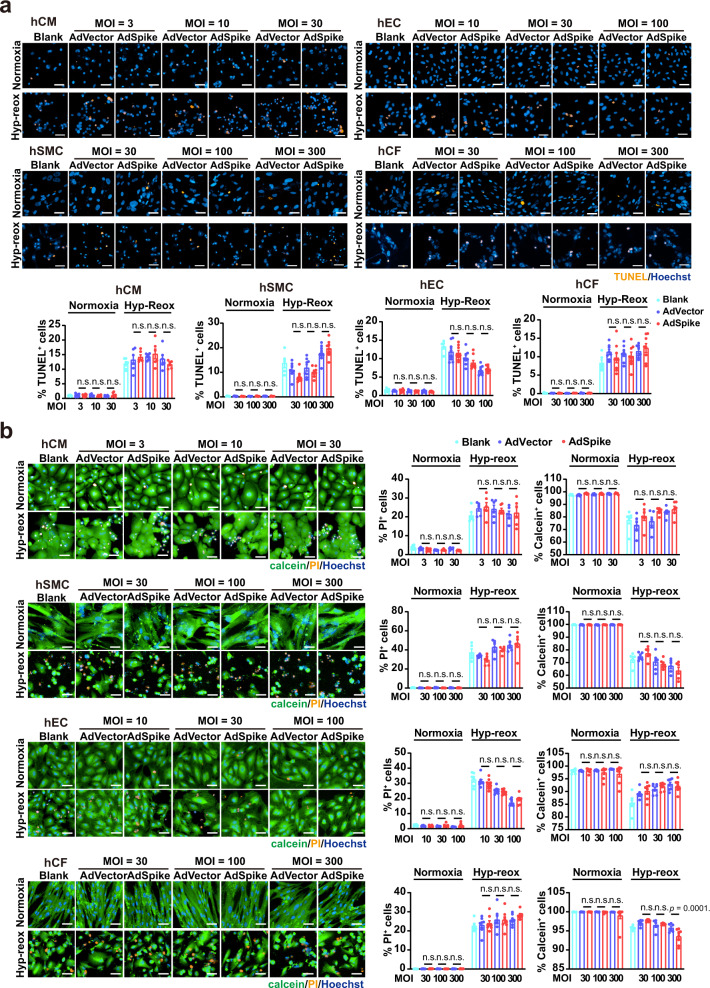
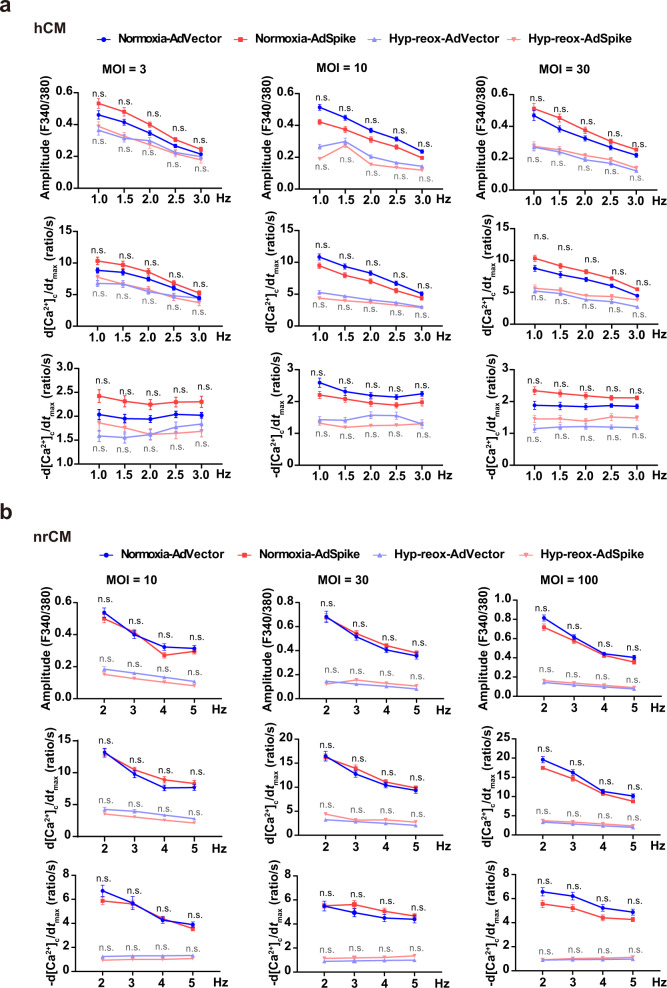
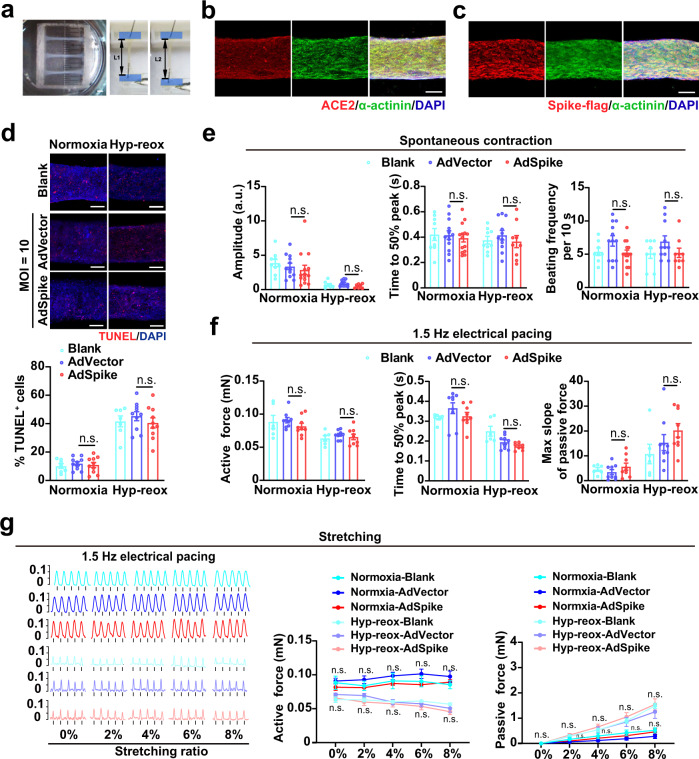
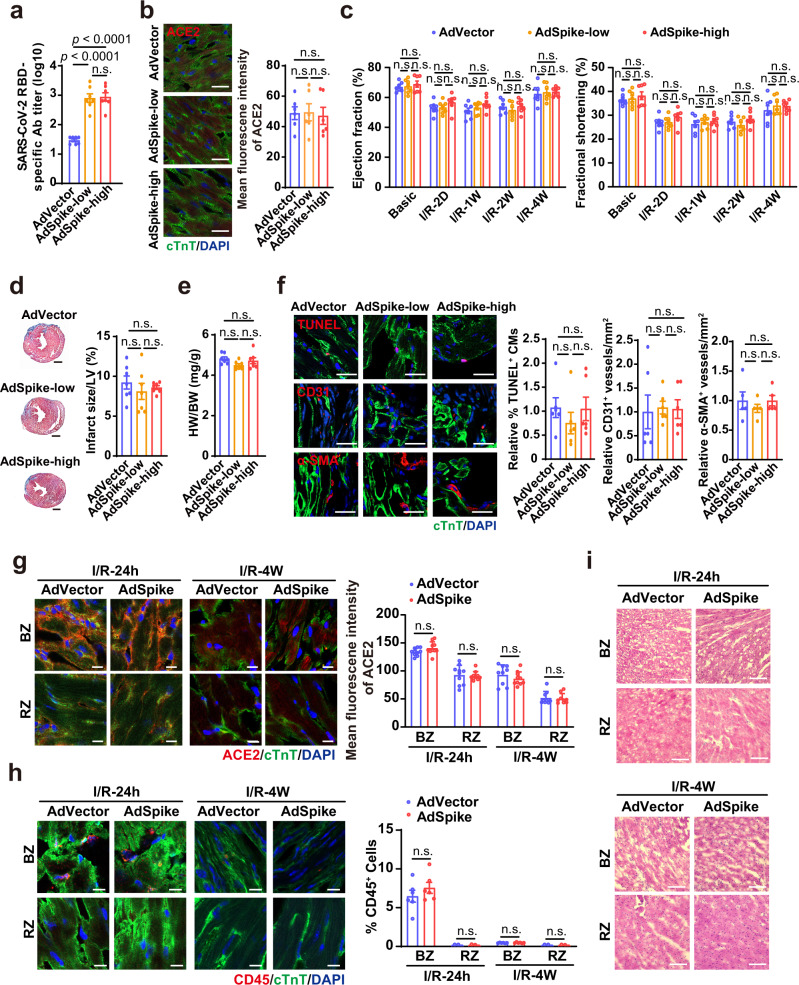
An unprecedented number of COVID-19 vaccination campaign are under way worldwide. The spike protein of SARS-CoV-2, which majorly binds to the host receptor angiotensin converting enzyme 2 (ACE2) for cell entry, is used by most of the vaccine as antigen. ACE2 is highly expressed in the heart and has been reported to be protective in multiple organs. Interaction of spike with ACE2 is known to reduce ACE2 expression and affect ACE2-mediated signal transduction. However, whether a spike-encoding vaccine will aggravate myocardial damage after a heart attack via affecting ACE2 remains unclear. Here, we demonstrate that cardiac ACE2 is up-regulated and protective after myocardial ischemia/reperfusion (I/R). Infecting human cardiac cells or engineered heart tissues with a spike-based adenovirus type-5 vectored COVID-19 vaccine (AdSpike) does not affect their survival and function, whether subjected to hypoxia-reoxygenation injury or not. Furthermore, AdSpike vaccination does not aggravate heart damage in wild-type or humanized ACE2 mice after I/R injury, even at a dose that is ten-fold higher as used in human. This study represents the first systematic evaluation of the safety of a leading COVID-19 vaccine under a disease context and may provide important information to ensure maximal protection from COVID-19 in patients with or at risk of heart diseases.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Expressions and significances of the angiotensin-converting enzyme 2 gene, the receptor of SARS-CoV-2 for COVID-19.Mol Biol Rep. 2020 Jun;47(6):4383-4392. doi: 10.1007/s11033-020-05478-4. Epub 2020 May 14. Mol Biol Rep. 2020. PMID: 32410141 Free PMC article.
-
Molecular Mimicry of the Viral Spike in the SARS-CoV-2 Vaccine Possibly Triggers Transient Dysregulation of ACE2, Leading to Vascular and Coagulation Dysfunction Similar to SARS-CoV-2 Infection.Viruses. 2023 Apr 25;15(5):1045. doi: 10.3390/v15051045. Viruses. 2023. PMID: 37243131 Free PMC article. Review.
-
Single-cell analysis of SARS-CoV-2 receptor ACE2 and spike protein priming expression of proteases in the human heart.Cardiovasc Res. 2020 Aug 1;116(10):1733-1741. doi: 10.1093/cvr/cvaa191. Cardiovasc Res. 2020. PMID: 32638018 Free PMC article.
-
The ACE2 expression in human heart indicates new potential mechanism of heart injury among patients infected with SARS-CoV-2.Cardiovasc Res. 2020 May 1;116(6):1097-1100. doi: 10.1093/cvr/cvaa078. Cardiovasc Res. 2020. PMID: 32227090 Free PMC article.
-
Angiotensin-Converting Enzyme 2 (ACE2) in the Pathogenesis of ARDS in COVID-19.Front Immunol. 2021 Dec 22;12:732690. doi: 10.3389/fimmu.2021.732690. eCollection 2021. Front Immunol. 2021. PMID: 35003058 Free PMC article. Review.
Cited by
-
Cardiac Disease Modeling with Engineered Heart Tissue.Handb Exp Pharmacol. 2023;281:235-255. doi: 10.1007/164_2023_681. Handb Exp Pharmacol. 2023. PMID: 37563250 Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
