

Wearable accelerometer-derived physical activity and incident disease
- PMID: 36056190
- PMCID: PMC9440134
- DOI: 10.1038/s41746-022-00676-9
Wearable accelerometer-derived physical activity and incident disease
Abstract
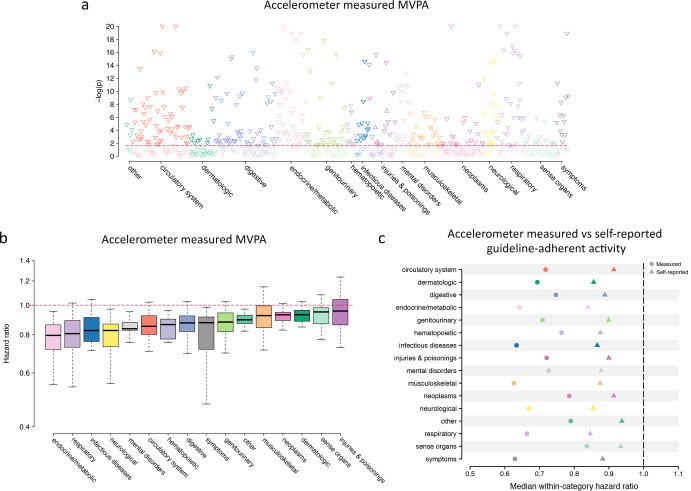
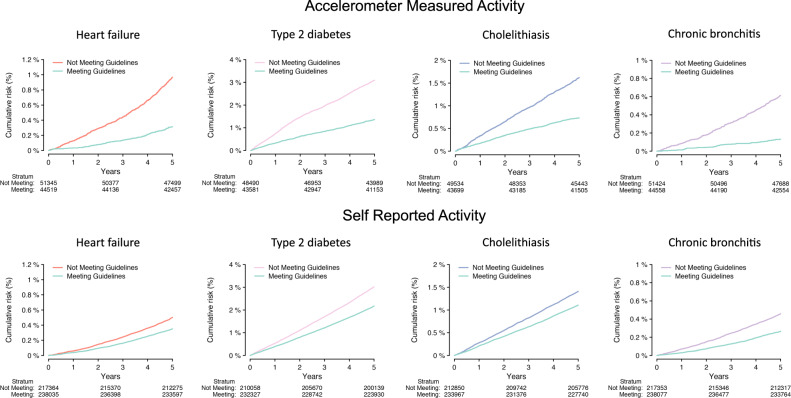
Physical activity is regarded as favorable to health but effects across the spectrum of human disease are poorly quantified. In contrast to self-reported measures, wearable accelerometers can provide more precise and reproducible activity quantification. Using wrist-worn accelerometry data from the UK Biobank prospective cohort study, we test associations between moderate-to-vigorous physical activity (MVPA) - both total MVPA minutes and whether MVPA is above a guideline-based threshold of ≥150 min/week-and incidence of 697 diseases using Cox proportional hazards models adjusted for age, sex, body mass index, smoking, Townsend Deprivation Index, educational attainment, diet quality, alcohol use, blood pressure, anti-hypertensive use. We correct for multiplicity at a false discovery rate of 1%. We perform analogous testing using self-reported MVPA. Among 96,244 adults wearing accelerometers for one week (age 62 ± 8 years), MVPA is associated with 373 (54%) tested diseases over a median 6.3 years of follow-up. Greater MVPA is overwhelmingly associated with lower disease risk (98% of associations) with hazard ratios (HRs) ranging 0.70-0.98 per 150 min increase in weekly MVPA, and associations spanning all 16 disease categories tested. Overall, associations with lower disease risk are enriched for cardiac (16%), digestive (14%), endocrine/metabolic (10%), and respiratory conditions (8%) (chi-square p < 0.01). Similar patterns are observed using the guideline-based threshold of ≥150 MVPA min/week. Some of the strongest associations with guideline-adherent activity include lower risks of incident heart failure (HR 0.65, 95% CI 0.55-0.77), type 2 diabetes (HR 0.64, 95% CI 0.58-0.71), cholelithiasis (HR 0.61, 95% CI 0.54-0.70), and chronic bronchitis (HR 0.42, 95% CI 0.33-0.54). When assessed within 456,374 individuals providing self-reported MVPA, effect sizes for guideline-adherent activity are substantially smaller (e.g., heart failure HR 0.84, 95% CI 0.80-0.88). Greater wearable device-based physical activity is robustly associated with lower disease incidence. Future studies are warranted to identify potential mechanisms linking physical activity and disease, and assess whether optimization of measured activity can reduce disease risk.
© 2022. The Author(s).
Conflict of interest statement
S.A.L. is a full-time employee of Novartis as of July 18, 2022. S.A.L. has received sponsored research support from Bristol Myers Squibb, Pfizer, Boehringer Ingelheim, Fitbit, Medtronic, Premier, and IBM, and has consulted for Bristol Myers Squibb, Pfizer, Blackstone Life Sciences, and Invitae. P.T.E. receives sponsored research support from Bayer AG and IBM Health and he has consulted for Bayer AG, Novartis, MyoKardia, and Quest Diagnostics. The remaining authors declare no competing interests.
Figures


References
-
- Elliott, A. D. et al. Association between physical activity and risk of incident arrhythmias in 402 406 individuals: evidence from the UK Biobank Cohort. Eur. Heart J. 10.1093/eurheartj/ehz897 (2020). - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
