

Impact of semaglutide on high-sensitivity C-reactive protein: exploratory patient-level analyses of SUSTAIN and PIONEER randomized clinical trials
- PMID: 36056351
- PMCID: PMC9440529
- DOI: 10.1186/s12933-022-01585-7
Impact of semaglutide on high-sensitivity C-reactive protein: exploratory patient-level analyses of SUSTAIN and PIONEER randomized clinical trials
Abstract
Background: Exploratory analysis to determine the effect of semaglutide versus comparators on high-sensitivity C-reactive protein (hsCRP) in subjects with type 2 diabetes.
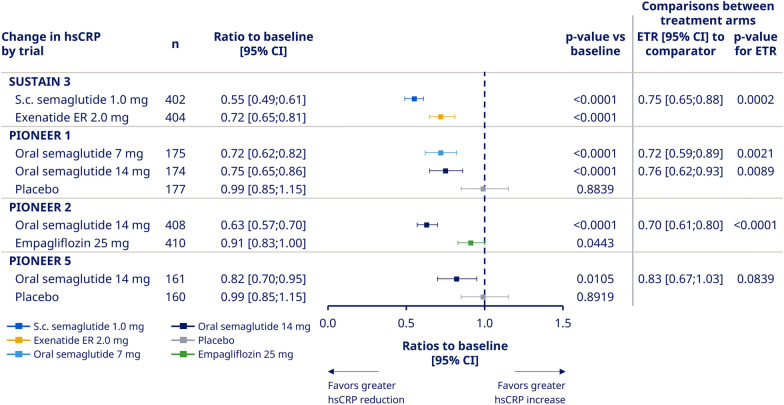
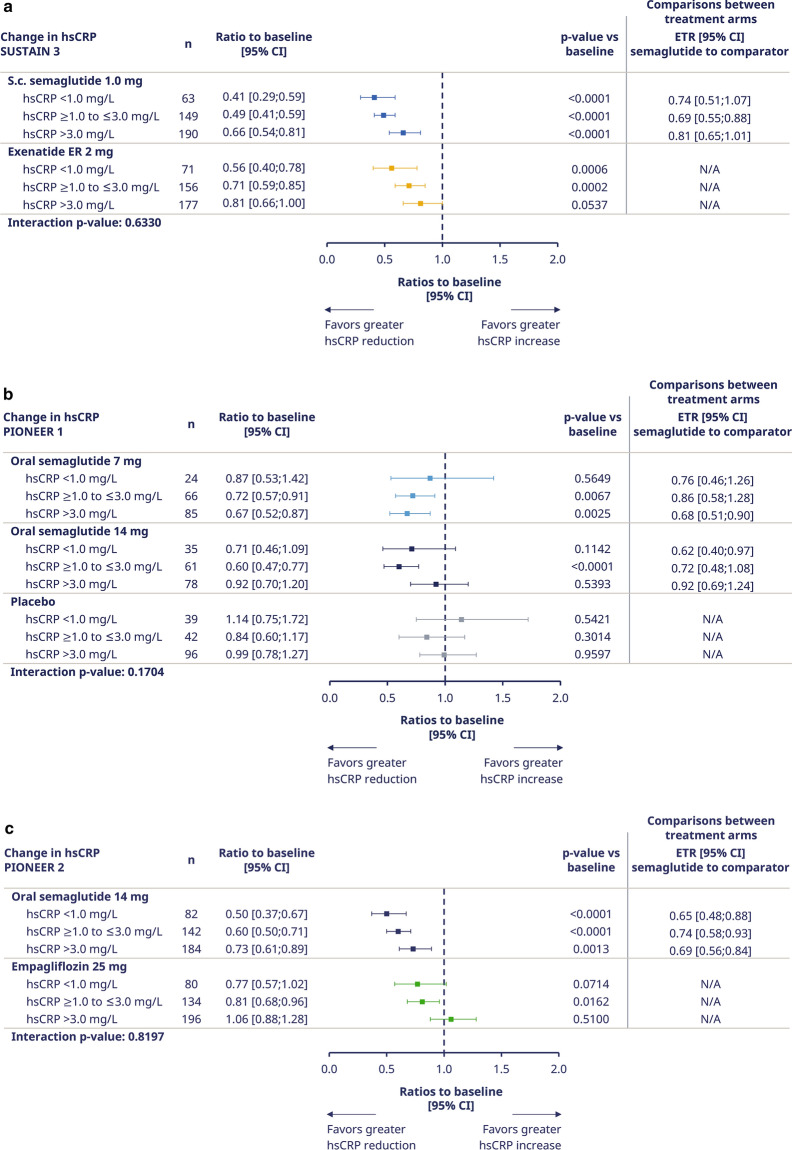
Methods: Trials of once-weekly subcutaneous (SUSTAIN 3) and once-daily oral (PIONEER 1, 2, 5) semaglutide with hsCRP data were analyzed. Subjects with type 2 diabetes (N = 2482) received semaglutide (n = 1328) or comparators (placebo, n = 339; exenatide extended-release, n = 405; empagliflozin, n = 410). hsCRP ratio to baseline at end-of-treatment was analyzed overall, by clinical cutoff (< 1.0, ≥ 1.0 to ≤ 3.0, or > 3.0 mg/L), by tertile, and by estimated glomerular filtration rate in PIONEER 5 (a trial which was conducted in a population with type 2 diabetes and chronic kidney disease [CKD]). Mediation analyses assessed the effect of change in glycated hemoglobin (HbA1c) and/or change in body weight (BW) on hsCRP reductions.
Results: Geometric mean baseline hsCRP was similar across trials (range 2.7-3.0 mg/L). Semaglutide reduced hsCRP levels by clinical cutoffs and tertiles from baseline to end-of-treatment in all trials versus comparators (estimated treatment ratios [ETRs] versus comparators: 0.70-0.76; p < 0.01) except versus placebo in PIONEER 5 (ETR [95% CI]: 0.83 [0.67-1.03]; p > 0.05). The effect of semaglutide on hsCRP was partially mediated (20.6-61.8%) by change in HbA1c and BW.
Conclusions: Semaglutide reduced hsCRP ratios-to-baseline versus comparators in subjects with type 2 diabetes (not significant with CKD). This effect was partially mediated via reductions in HbA1c and BW and potentially by a direct effect of semaglutide. Semaglutide appears to have an anti-inflammatory effect, which is being further investigated in ongoing trials.
Trial registrations: ClinicalTrials.gov identifiers: NCT01885208 (first registered June 2013), NCT02906930 (first registered September 2016), NCT02863328 (first registered August 2016), NCT02827708 (first registered July 2016).
Keywords: Body weight; Chronic kidney disease; GLP-1RAs; HbA1c; High-sensitivity C-reactive protein; Inflammation; PIONEER; SUSTAIN; Semaglutide; Type 2 diabetes.
© 2022. The Author(s).
Conflict of interest statement
OM reports personal fees for advisory board consultancy and speaker’s bureau from AstraZeneca, Boehringer Ingelheim, Eli Lilly, MSD, Novo Nordisk, and Sanofi; and research grant support from AstraZeneca and Novo Nordisk. MC reports being a partner at Clifton Medical Centre, a director at RIO Weight Management, Ltd, and a consultant for LighterLife and McDonald’s; he also reports research funding from Abbott, Boehringer Ingelheim/Lilly Alliance, Janssen, MSD, and Novo Nordisk; advisory board consultancy, consultancy and honoraria from Abbott, Boehringer Ingelheim/Lilly Alliance, and Novo Nordisk; and meeting support from Boehringer Ingelheim/Lilly Alliance and Novo Nordisk. ADR, SR, and PW are full-time employees of Novo Nordisk; SR also owns shares in Novo Nordisk. JR reports research funding from Applied Therapeutics Inc., Boehringer Ingelheim, Eli Lilly, Genentech, GlaxoSmithKline, Hanmi, Intarcia, Janssen, Lexicon, Merck, Metacrine, Novo Nordisk, Novartis, Oramed, Pfizer, and Sanofi; and advisory board consultancy, consultancy, and honoraria from Applied Therapeutics Inc., Boehringer Ingelheim, Eli Lilly, Hanmi, Intarcia, Janssen, Novo Nordisk, Oramed, Sanofi, and Zealand.
Figures


References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
