

Clinical complexity and impact of the ABC (Atrial fibrillation Better Care) pathway in patients with atrial fibrillation: a report from the ESC-EHRA EURObservational Research Programme in AF General Long-Term Registry
- PMID: 36056426
- PMCID: PMC9440492
- DOI: 10.1186/s12916-022-02526-7
Clinical complexity and impact of the ABC (Atrial fibrillation Better Care) pathway in patients with atrial fibrillation: a report from the ESC-EHRA EURObservational Research Programme in AF General Long-Term Registry
Abstract
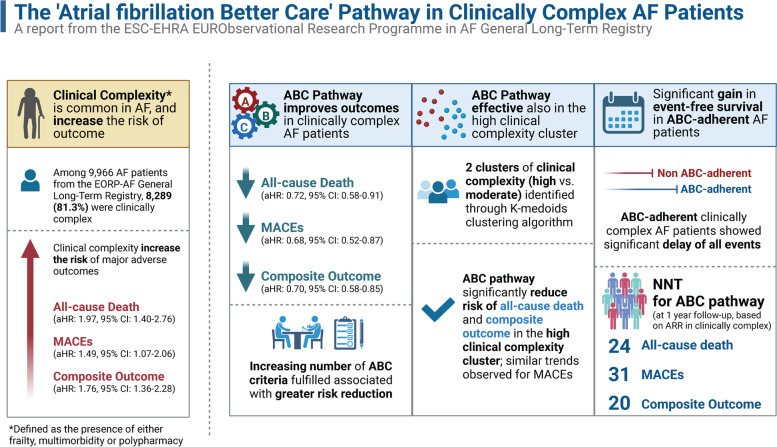
Background: Clinical complexity is increasingly prevalent among patients with atrial fibrillation (AF). The 'Atrial fibrillation Better Care' (ABC) pathway approach has been proposed to streamline a more holistic and integrated approach to AF care; however, there are limited data on its usefulness among clinically complex patients. We aim to determine the impact of ABC pathway in a contemporary cohort of clinically complex AF patients.
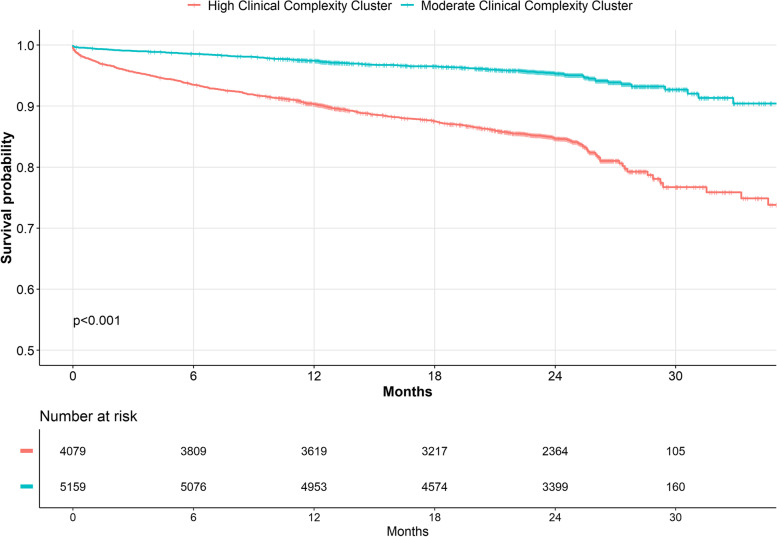
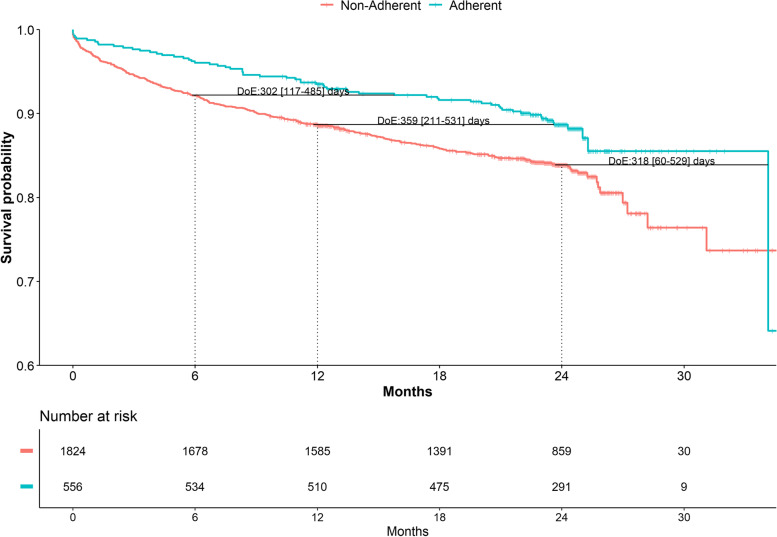
Methods: From the ESC-EHRA EORP-AF General Long-Term Registry, we analysed clinically complex AF patients, defined as the presence of frailty, multimorbidity and/or polypharmacy. A K-medoids cluster analysis was performed to identify different groups of clinical complexity. The impact of an ABC-adherent approach on major outcomes was analysed through Cox-regression analyses and delay of event (DoE) analyses.
Results: Among 9966 AF patients included, 8289 (83.1%) were clinically complex. Adherence to the ABC pathway in the clinically complex group reduced the risk of all-cause death (adjusted HR [aHR]: 0.72, 95%CI 0.58-0.91), major adverse cardiovascular events (MACEs; aHR: 0.68, 95%CI 0.52-0.87) and composite outcome (aHR: 0.70, 95%CI: 0.58-0.85). Adherence to the ABC pathway was associated with a significant reduction in the risk of death (aHR: 0.74, 95%CI 0.56-0.98) and composite outcome (aHR: 0.76, 95%CI 0.60-0.96) also in the high-complexity cluster; similar trends were observed for MACEs. In DoE analyses, an ABC-adherent approach resulted in significant gains in event-free survival for all the outcomes investigated in clinically complex patients. Based on absolute risk reduction at 1 year of follow-up, the number needed to treat for ABC pathway adherence was 24 for all-cause death, 31 for MACEs and 20 for the composite outcome.
Conclusions: An ABC-adherent approach reduces the risk of major outcomes in clinically complex AF patients. Ensuring adherence to the ABC pathway is essential to improve clinical outcomes among clinically complex AF patients.
Keywords: Atrial fibrillation; Clinical complexity; Integrated management; Outcomes.
© 2022. The Author(s).
Conflict of interest statement
Figures
References
-
- Woolford SJ, Aggarwal P, Sheikh CJ, Patel HP. Frailty, multimorbidity and polypharmacy. Medicine (United Kingdom) 2021;49:166–172.
-
- Proietti M, Cesari M. Describing the relationship between atrial fibrillation and frailty: clinical implications and open research questions. Exp Gerontol. 2021;152:111455. - PubMed
