

Stroke-Heart Syndrome: Recent Advances and Challenges
- PMID: 36056731
- PMCID: PMC9496419
- DOI: 10.1161/JAHA.122.026528
Stroke-Heart Syndrome: Recent Advances and Challenges
Abstract
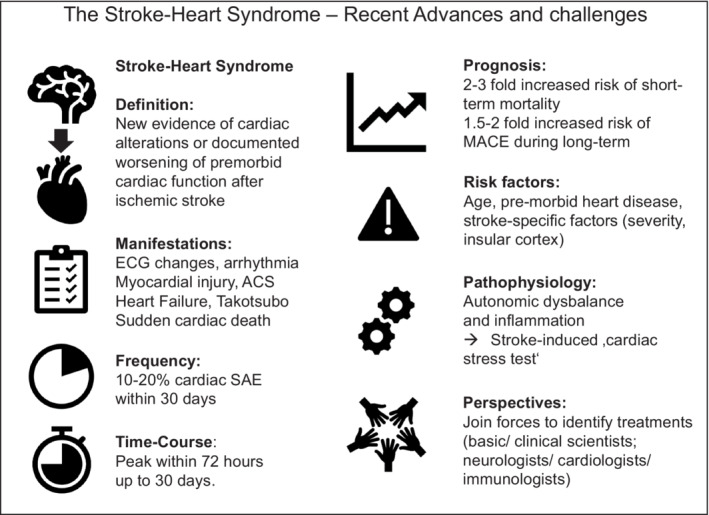
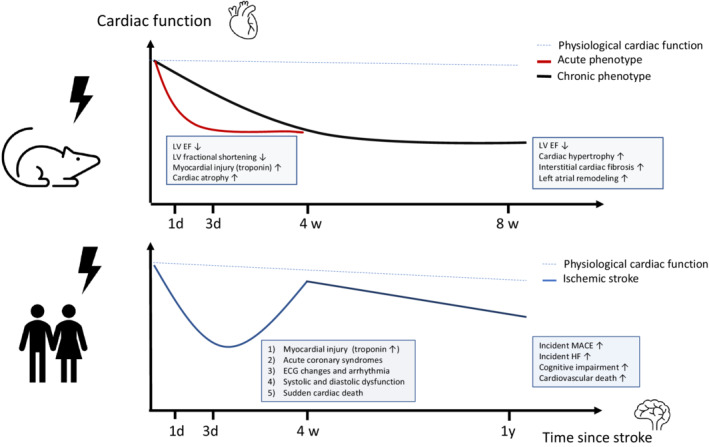
After ischemic stroke, there is a significant burden of cardiovascular complications, both in the acute and chronic phase. Severe adverse cardiac events occur in 10% to 20% of patients within the first few days after stroke and comprise a continuum of cardiac changes ranging from acute myocardial injury and coronary syndromes to heart failure or arrhythmia. Recently, the term stroke-heart syndrome was introduced to provide an integrated conceptual framework that summarizes neurocardiogenic mechanisms that lead to these cardiac events after stroke. New findings from experimental and clinical studies have further refined our understanding of the clinical manifestations, pathophysiology, and potential long-term consequences of the stroke-heart syndrome. Local cerebral and systemic mediators, which mainly involve autonomic dysfunction and increased inflammation, may lead to altered cardiomyocyte metabolism, dysregulation of (tissue-resident) leukocyte populations, and (micro-) vascular changes. However, at the individual patient level, it remains challenging to differentiate between comorbid cardiovascular conditions and stroke-induced heart injury. Therefore, further research activities led by joint teams of basic and clinical researchers with backgrounds in both cardiology and neurology are needed to identify the most relevant therapeutic targets that can be tested in clinical trials.
Keywords: brain–heart axis; heart; inflammation; outcomes; stroke.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
