

Global Burden, Regional Differences, Trends, and Health Consequences of Medication Nonadherence for Hypertension During 2010 to 2020: A Meta-Analysis Involving 27 Million Patients
- PMID: 36056737
- PMCID: PMC9496433
- DOI: 10.1161/JAHA.122.026582
Global Burden, Regional Differences, Trends, and Health Consequences of Medication Nonadherence for Hypertension During 2010 to 2020: A Meta-Analysis Involving 27 Million Patients
Abstract
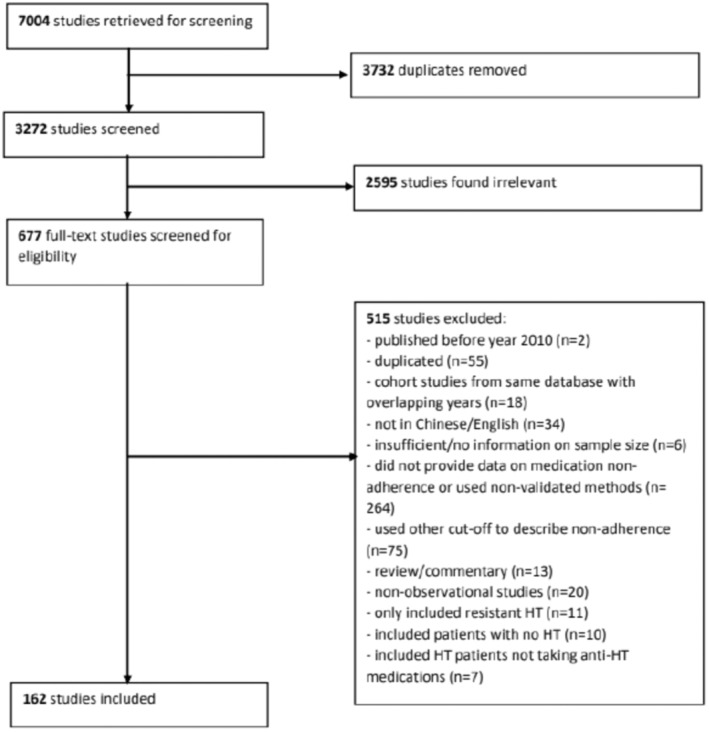
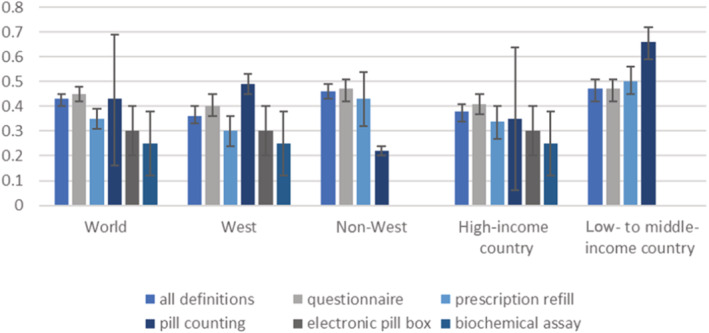
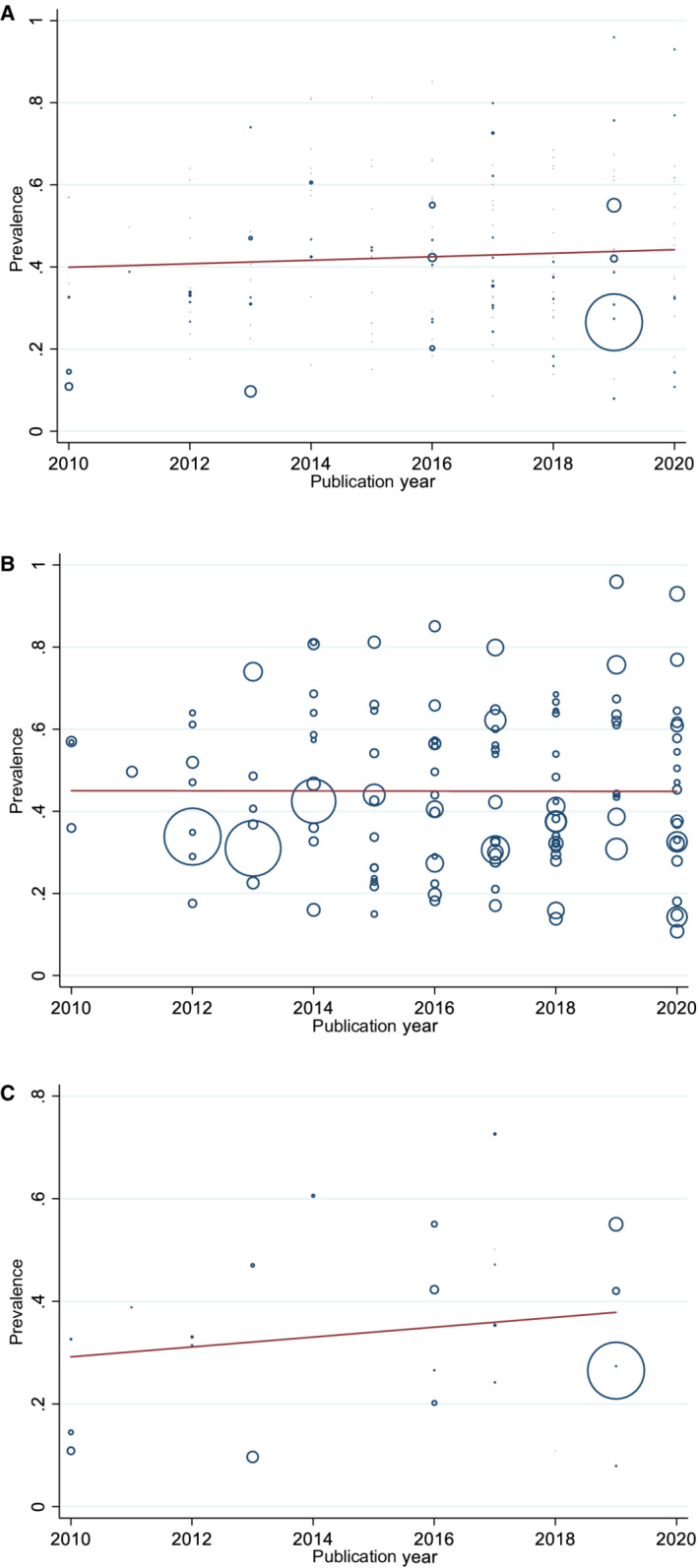
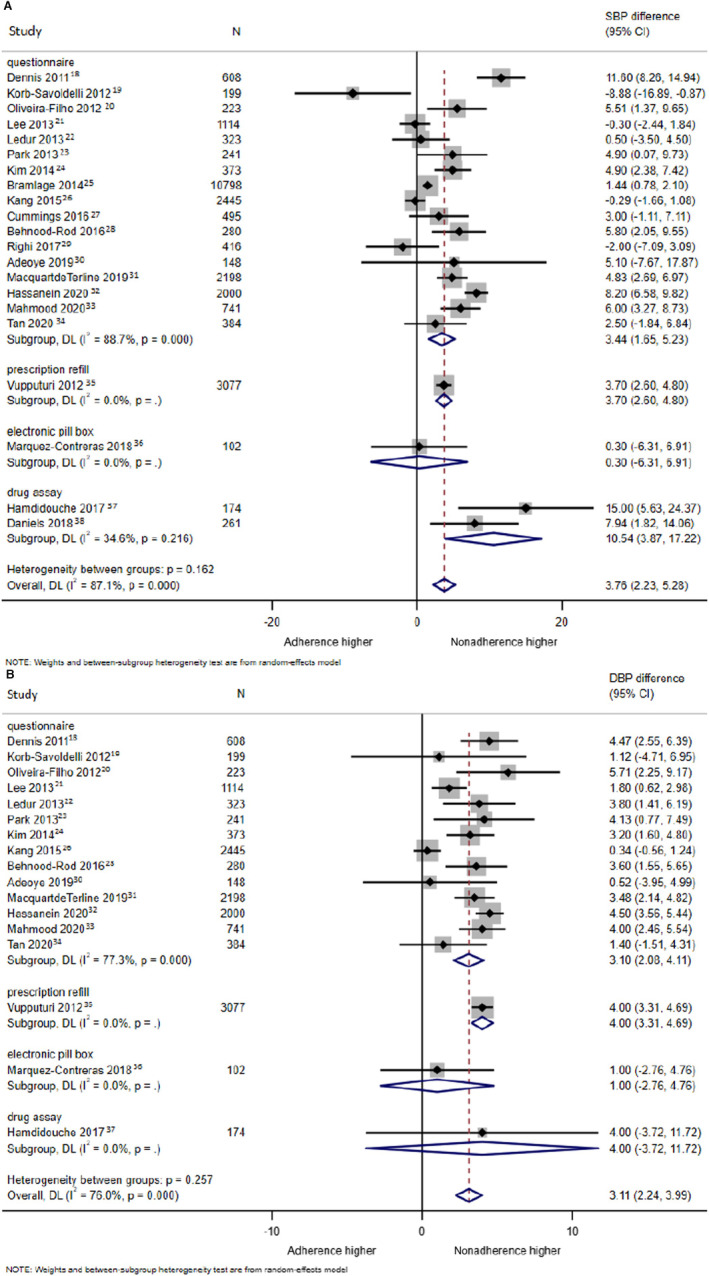
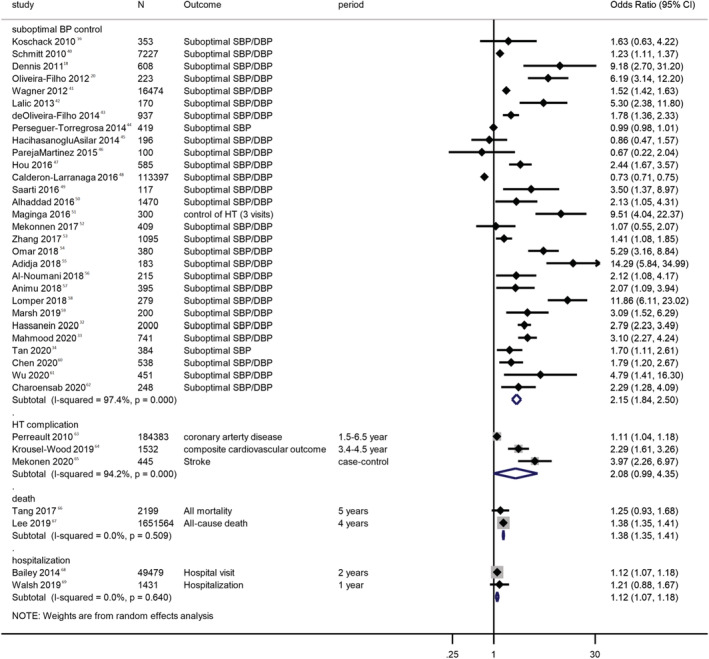
Background Nonadherence to antihypertensive medications is the leading cause of poor blood pressure control and thereby cardiovascular diseases and mortality worldwide. Methods and Results We investigated the global epidemiology, regional differences, and trend of antihypertensive medication nonadherence via a systematic review and meta-analyses of data from 2010 to 2020. Multiple medical databases and clinicaltrials.gov were searched for articles. Observational studies reporting the proportion of patients with anti-hypertensive medication nonadherence were included. The proportion of nonadherence, publication year, year of first recruitment, country, and health outcomes attributable to antihypertensive medication nonadherence were extracted. Two reviewers screened abstracts and full texts, classified countries according to levels of income and locations, and extracted data. The Joanna Briggs Institute prevalence critical appraisal tool was used to rate the included studies. Prevalence meta-analyses were conducted using a fixed-effects model, and trends in prevalence were analyzed using meta-regression. The certainty of evidence concerning the effect of health consequences of nonadherence was rated according to Grading of Recommendations, Assessment, Development and Evaluations. A total of 161 studies were included. Subject to different detection methods, the global prevalence of anti-hypertensive medication nonadherence was 27% to 40%. Nonadherence was more prevalent in low- to middle-income countries than in high-income countries, and in non-Western countries than in Western countries. No significant trend in prevalence was detected between 2010 and 2020. Patients with antihypertensive medication nonadherence had suboptimal blood pressure control, complications from hypertension, all-cause hospitalization, and all-cause mortality. Conclusions While high prevalence of anti-hypertensive medication nonadherence was detected worldwide, higher prevalence was detected in low- to middle-income and non-Western countries. Interventions are urgently required, especially in these regions. Current evidence is limited by high heterogeneity. Registration URL: www.crd.york.ac.uk/prospero/; Unique identifier: CRD42021259860.
Keywords: adherence; compliance; hypertension; meta‐analyses; prevalence.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
