

Clinical characteristics and comparison of longitudinal qPCR results from different specimen types in a cohort of ambulatory and hospitalized patients infected with monkeypox virus
- PMID: 36057206
- PMCID: PMC9528238
- DOI: 10.1016/j.jcv.2022.105254
Clinical characteristics and comparison of longitudinal qPCR results from different specimen types in a cohort of ambulatory and hospitalized patients infected with monkeypox virus
Abstract
Background: The ongoing monkeypox virus outbreak includes at least 7553 confirmed cases in previously non-endemic countries worldwide as of July 2022. Clinical presentation has been reported as highly variable, sometimes lacking classically described systemic symptoms, and only small numbers of cutaneous lesions in most patients. The aim of this study was to compare clinical data with longitudinal qPCR results from lesion swabs, oropharyngeal swabs and blood in a well characterized patient cohort.
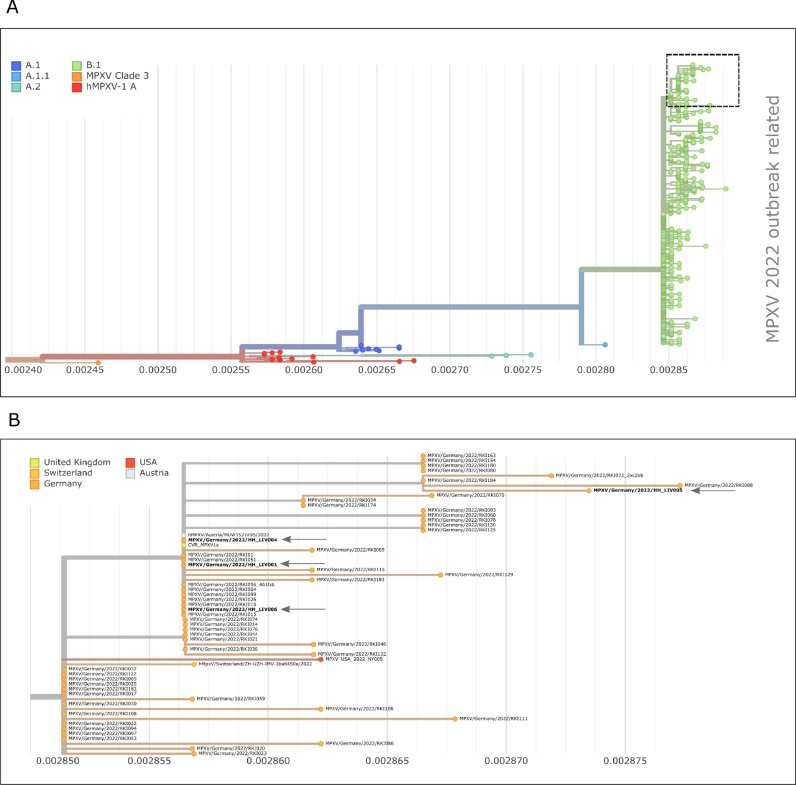
Methods: 16 male patients (5 hospitalized, 11 outpatients) were included in the study cohort and serial testing for monkeypox virus-DNA carried out in various materials throughout the course of disease. Laboratory analysis included quantitative PCR, next-generation sequencing, immunofluorescence tests and virus isolation in cell culture.
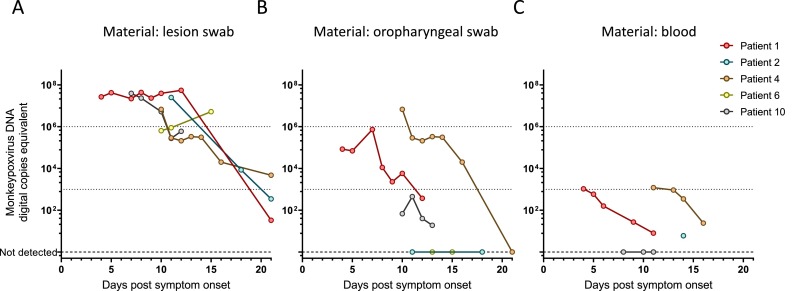
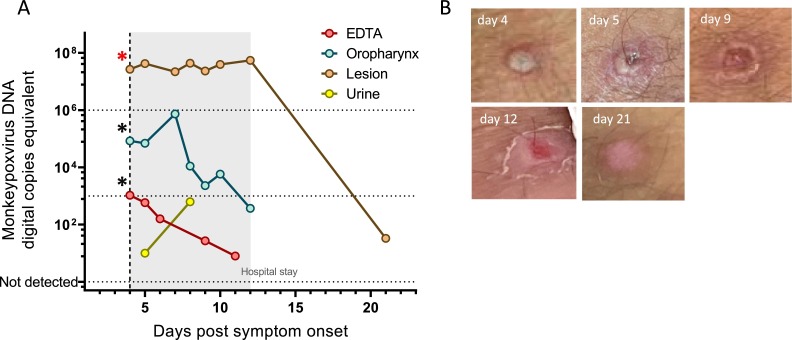
Results: All patients were male, between age 20 and 60, and self-identified as men having sex with men. Two had a known HIV infection, coinciding with an increased number of lesions and viral DNA detectable in blood. In initial- and serial testing, lesion swabs yielded viral DNA-loads at, or above 106 cp/ml and only declined during the third week. Oropharyngeal swabs featured lower viral loads and returned repeatedly negative in some cases. Viral culture was successful only from lesion swabs but not from oropharyngeal swabs or plasma.
Discussion: The data presented underscore the reliability of lesion swabs for monkeypox virus-detection, even in later stages of the disease. Oropharyngeal swabs and blood samples alone carry the risk of false negative results, but may hold value in pre-/asymptomatic cases or viral load monitoring, respectively.
Keywords: Clinical cohort; Clinical specimens; Monkeypox virus; Viral load kinetics; qPCR.
Copyright © 2022. Published by Elsevier B.V.
Conflict of interest statement
Declaration of Competing Interest ML and DN received speaker honoraria and related travel expenses from Roche Diagnostics.All other authors declare no conflict of interest.
Figures
References
-
- ECDC Monkeypox multi-country outbreak, first update –8 July 2022. ECDC Website. 2022
-
- Kozlov M. Monkeypox goes global: why scientists are on alert. Nature. 2022;606:15–16. - PubMed
-
- Antinori A., Mazzotta V., Vita S., Carletti F., Tacconi D., Lapini L.E., D'Abramo A., Cicalini S., Lapa D., Pittalis S.,., Puro V., Rivano Capparuccia M., Giombini E., Gruber C.E.M., Garbuglia A.R., Marani A., Vairo F., Girardi E., Vaia F., Nicastri E., Group tIM Epidemiological, clinical and virological characteristics of four cases of monkeypox support transmission through sexual contact, Italy, May 2022. Eurosurveillance. 2022;27 - PMC - PubMed
-
- Vivancos R., Anderson C., Blomquist P., Balasegaram S., Bell A., Bishop L., Brown C.S., Chow Y., Edeghere O., Florence I., Logan S., Manley P., Crowe W., McAuley A., Shankar A.G., Mora-Peris B., Paranthaman K., Prochazka M., Ryan C., Simons D., Vipond R., Byers C., Watkins N.A., team UMIM. Welfare W., Whittaker E., Dewsnap C., Wilson A., Young Y., Chand M., Riley S., Hopkins S. Community transmission of monkeypox in the United Kingdom, April to May 2022. Eurosurveillance. 2022;27 - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
