

Ictal apnea: A prospective monocentric study in patients with epilepsy
- PMID: 36057450
- PMCID: PMC9826458
- DOI: 10.1111/ene.15547
Ictal apnea: A prospective monocentric study in patients with epilepsy
Abstract
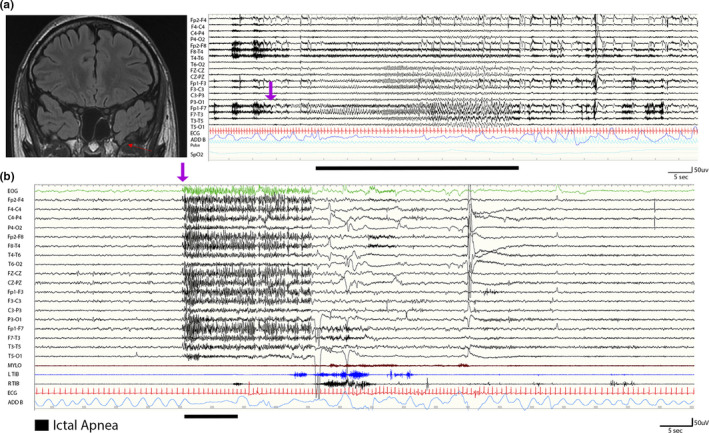
Background and purpose: Ictal respiratory disturbances have increasingly been reported, in both generalized and focal seizures, especially involving the temporal lobe. Recognition of ictal breathing impairment has gained importance for the risk of sudden unexpected death in epilepsy (SUDEP). The aim of this study was to evaluate the incidence of ictal apnea (IA) and related hypoxemia during seizures.
Methods: We collected and analyzed electroclinical data from consecutive patients undergoing long-term video-electroencephalographic (video-EEG) monitoring with cardiorespiratory polygraphy. Patients were recruited at the epilepsy monitoring unit of the Civil Hospital of Baggiovara, Modena Academic Hospital, from April 2020 to February 2022.
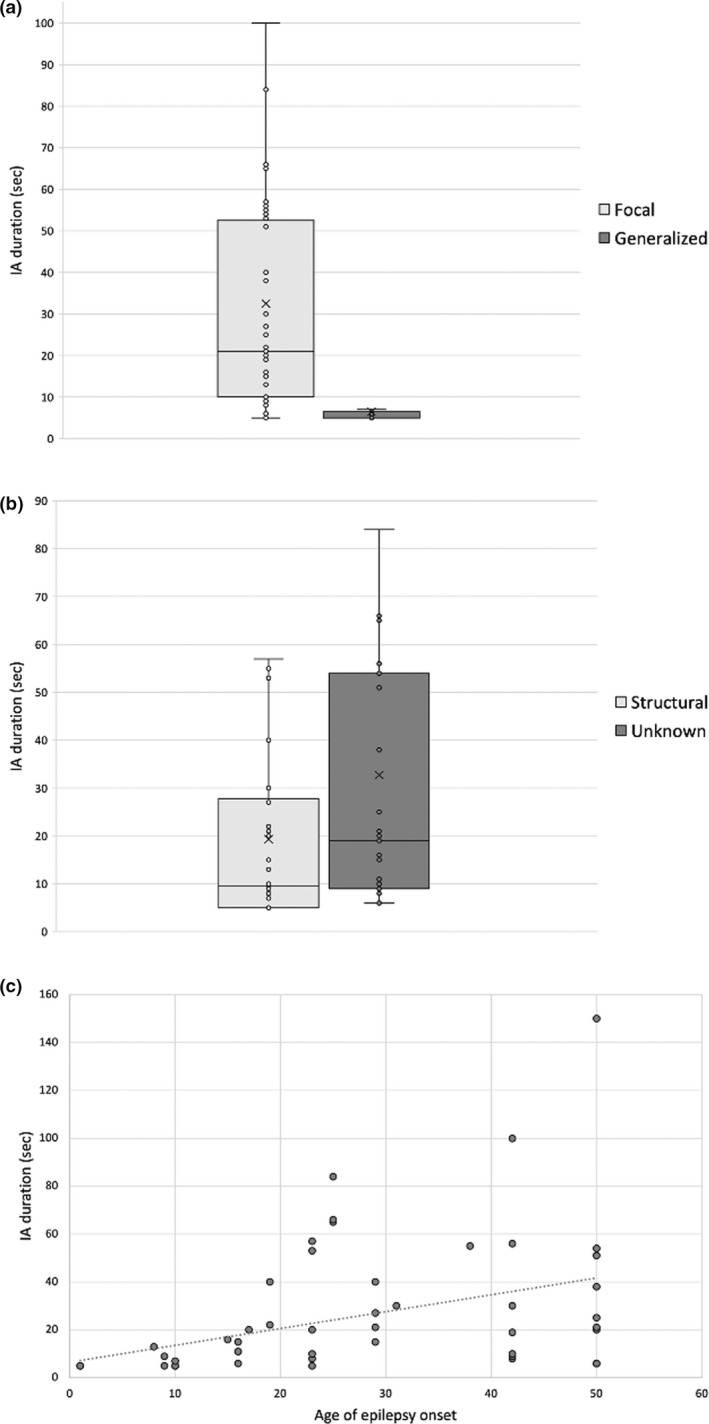
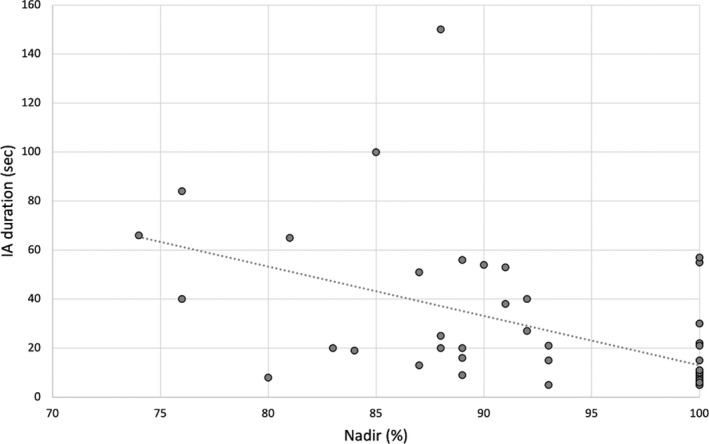
Results: A total of 552 seizures were recorded in 63 patients. IA was observed in 57 of 552 (10.3%) seizures in 16 of 63 (25.4%) patients. Thirteen (81.2%) patients had focal seizures, and 11 of 16 patients showing IA had a diagnosis of temporal lobe epilepsy; two had a diagnosis of frontal lobe epilepsy and three of epileptic encephalopathy. Apnea agnosia was reported in all seizure types. Hypoxemia was observed in 25 of 57 (43.9%) seizures with IA, and the severity of hypoxemia was related to apnea duration. Apnea duration was significantly associated with epilepsy of unknown etiology (magnetic resonance imaging negative) and with older age at epilepsy onset (p < 0.001).
Conclusions: Ictal respiratory changes are a frequent clinical phenomenon, more likely to occur in focal epilepsies, although detected even in patients with epileptic encephalopathy. Our findings emphasize the need for respiratory polygraphy during long-term video-EEG monitoring for diagnostic and prognostic purposes, as well as in relation to the potential link of ictal apnea with the SUDEP risk.
Keywords: central apnea; electroencephalography; hypoxia; sudden unexpected death in epilepsy; temporal lobe epilepsy.
© 2022 The Authors. European Journal of Neurology published by John Wiley & Sons Ltd on behalf of European Academy of Neurology.
Conflict of interest statement
S.M. has received research grant support from the Ministry of Health and the nonprofit organization Fondazione Cassa di Risparmio di Modena; he has received personal compensation as a scientific advisory board member for UCB and Eisai. A.E.V. has received personal compensation as a scientific advisory board member for Angelini Pharma. The other authors report no conflict of interest.
Figures
References
-
- Blum AS. Respiratory physiology of seizures clinical findings of ictal respiratory changes. J Clin Neurophysiol. 2009;26:309‐315. - PubMed
-
- Jackson JH. On asphyxia in slight epileptic paroxysms: on the symptomatology of slight epileptic fits supposed to depend on discharge‐lesions of the uncinate gyrus. Lancet. 1899;1:79‐80.
-
- Coulter DL. Partial seizures with apnea and bradycardia. Arch Neurol. 1984;41:173‐174. http://archneur.jamanetwork.com/ - PubMed
-
- Singh B, Al Shahwan SA, Al Deeb SM. Partial seizures presenting as life‐ threatening apnea. Epilepsia. 1993;34(5):901‐903. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
