

Discomfort improvement for critically ill patients using electronic relaxation devices: results of the cross-over randomized controlled trial E-CHOISIR (Electronic-CHOIce of a System for Intensive care Relaxation)
- PMID: 36057612
- PMCID: PMC9440448
- DOI: 10.1186/s13054-022-04136-4
Discomfort improvement for critically ill patients using electronic relaxation devices: results of the cross-over randomized controlled trial E-CHOISIR (Electronic-CHOIce of a System for Intensive care Relaxation)
Erratum in
-
Publisher Correction to: Discomfort improvement for critically ill patients using electronic relaxation devices: results of the cross‑over randomized controlled trial E‑CHOISIR (Electronic‑CHOIce of a System for Intensive care Relaxation).Crit Care. 2022 Sep 26;26(1):291. doi: 10.1186/s13054-022-04169-9. Crit Care. 2022. PMID: 36163028 Free PMC article. No abstract available.
Abstract
Purpose: To assess the impact of different electronic relaxation devices on common stressful patient symptoms experienced in intensive care unit (ICU).
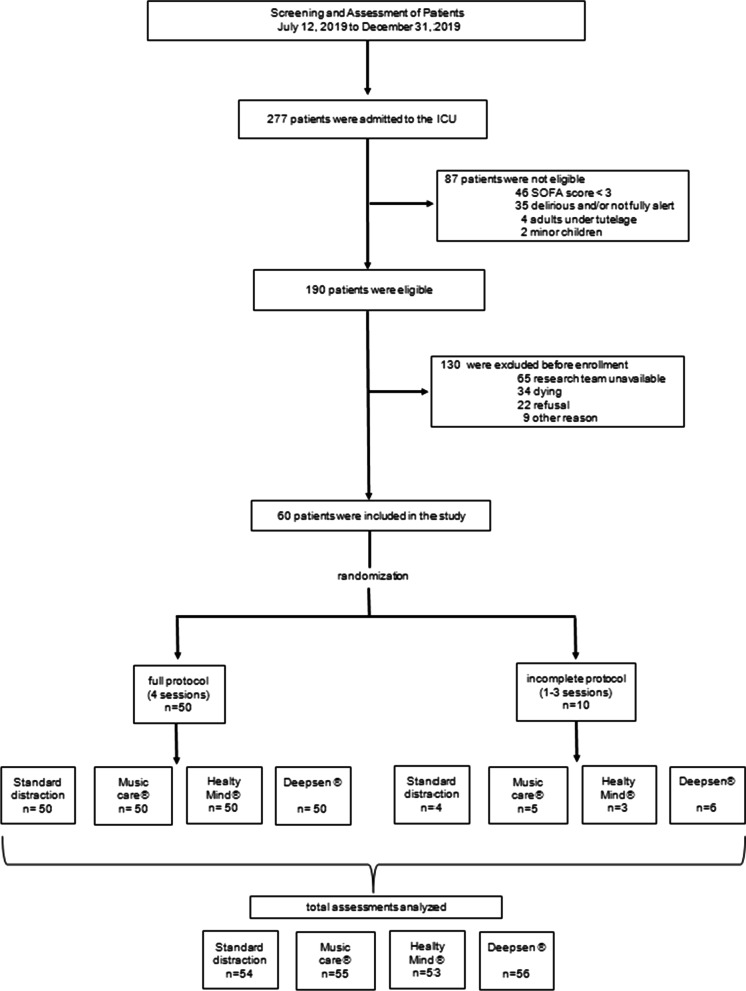
Methods: Sixty critically ill patients were enrolled in four relaxation sessions using a randomized cross-over design: standard relaxation (TV/radio), music therapy (MUSIC-CARE©), and two virtual reality systems using either real motion pictures (DEEPSEN©) or synthetic motion pictures (HEALTHY-MIND©). The goal was to determine which device was the best to reduce overall patient discomfort intensity (0-10 Numeric Rating Scale (NRS); primary endpoint). Secondary endpoints were specific stressful symptoms (pain, anxiety, dyspnea, thirst, and lack of rest feeling) and stress response measured by Analgesia/Nociception Index (ANI). Multivariate mixed-effect analysis was used, taking into account patient characteristics and multiple measurements.
Results: Fifty patients followed the full research protocol, and ten patients did at least one research planned session of relaxation. HEALTHY-MIND© was associated with a significant decrease in overall discomfort, the primary endpoint (median NRS = 4[2-6] vs. 2[0-5]; p = 0.01, mixed-effect model), accompanied by a significant decrease in stress response (increase in ANI, secondary endpoint; p < 0.01). Regarding other secondary endpoints, each of the two virtual reality systems was associated with a decrease in anxiety (p < 0.01), while HEALTHY-MIND© was associated also with a decrease in pain (p = 0.001) and DEEPSEN© with a decrease in lack of rest (p = 0.01). Three incidents (claustrophobia/dyspnea/agitation) were reported among 109 virtual reality sessions. Cybersickness was rare (NRS = 0[0-0]).
Conclusion: Electronic relaxation therapy is a promising, safe, and effective non-pharmacological solution that can be used to improve overall discomfort in alert and non-delirious ICU patients. Its effectiveness depends on technical characteristics (virtual reality using a synthetic imagined world versus a real world or music therapy alone without virtual reality), as well as the type of symptoms.
Keywords: Intensive care; Music therapy; Non-pharmacological therapies; Supportive care; Virtual reality.
© 2022. The Author(s).
Conflict of interest statement
Samir Jaber reports consulting fees from Drager, Xenios, Medtronic and Fisher and Paykel. Other authors declare no conflicts of interest. The music therapy system was purchased by the hospital several years before the study. The two virtual reality systems were lent to the hospital by the manufacturers for a free test. Manufacturers gave their consent for the evaluation study but had strictly no implication on the study design, data analysis, and study reporting.
Figures

References
-
- Devlin JW, Skrobik Y, Gelinas C, Needham DM, Slooter AJC, Pandharipande PP, Watson PL, Weinhouse GL, Nunnally ME, Rochwerg B, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018;46(9):e825–e873. doi: 10.1097/CCM.0000000000003299. - DOI - PubMed
-
- de Jong A, Molinari N, de Lattre S, Gniadek C, Carr J, Conseil M, Susbielles MP, Jung B, Jaber S, Chanques G. Decreasing severe pain and serious adverse events while moving intensive care unit patients: a prospective interventional study (the NURSE-DO project) Crit Care. 2013;17(2):R74. doi: 10.1186/cc12683. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
