

Interrupted-time-series analysis of the immediate impact of COVID-19 mitigation measures on preterm birth in China
- PMID: 36057724
- PMCID: PMC9440464
- DOI: 10.1038/s41467-022-32814-y
Interrupted-time-series analysis of the immediate impact of COVID-19 mitigation measures on preterm birth in China
Abstract
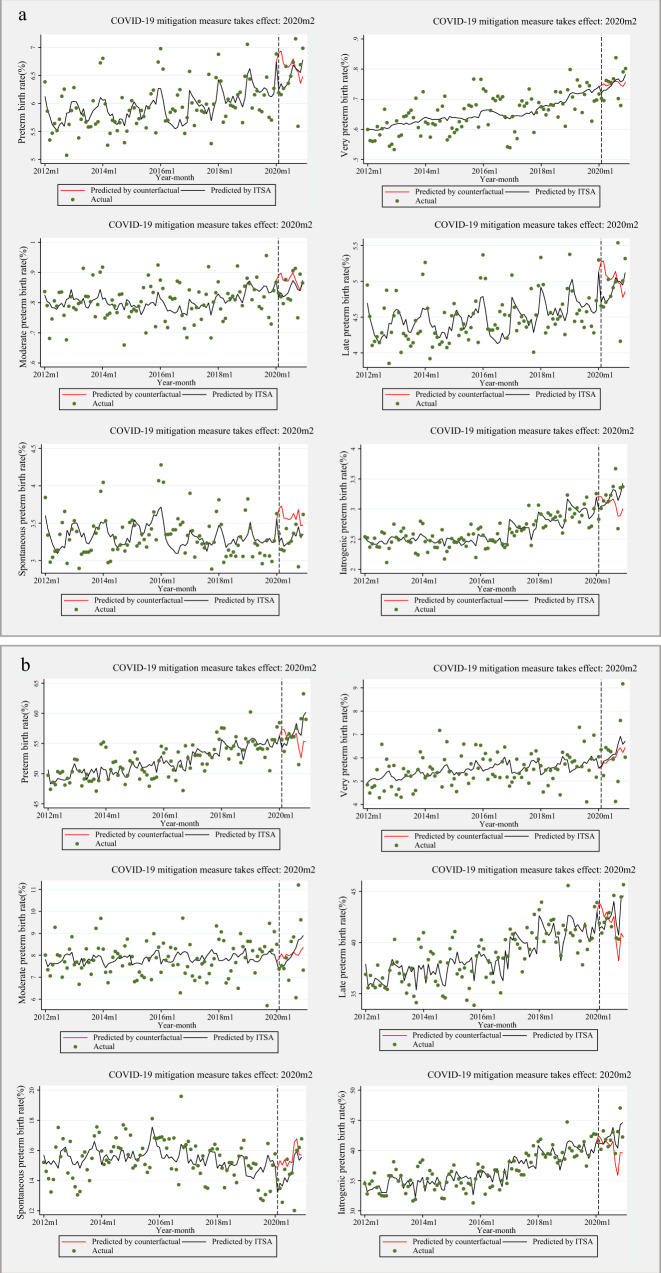
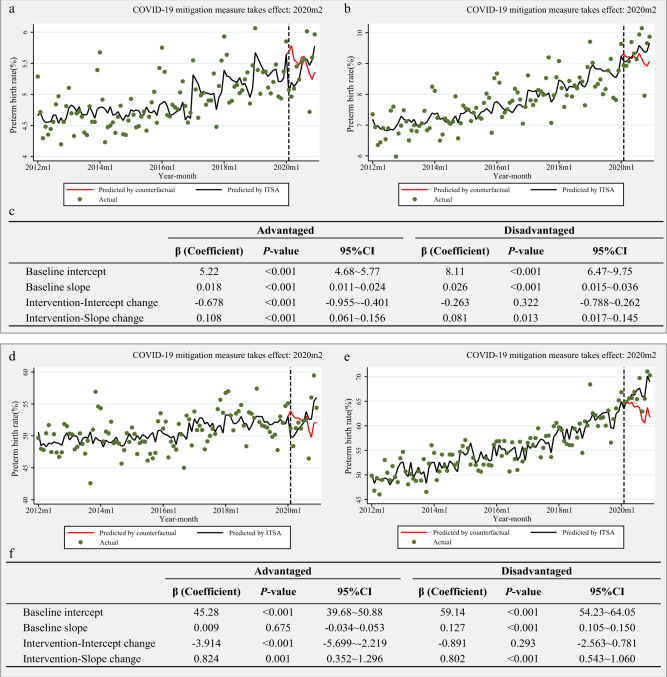
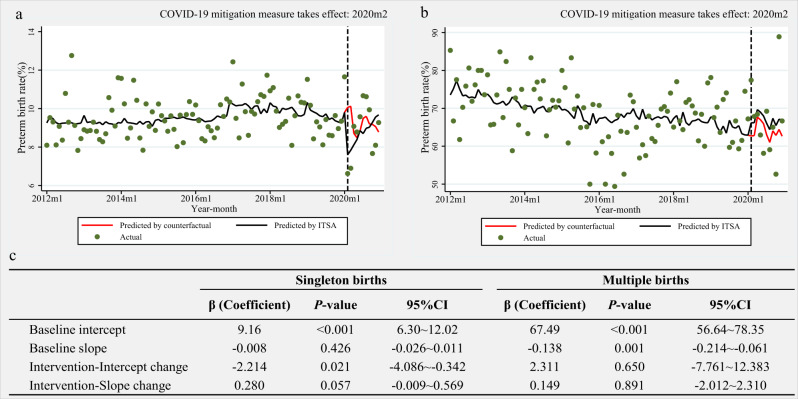
Preliminary evidence from China and other countries has suggested that coronavirus disease 2019 (COVID-19) mitigation measures have caused a decline in preterm births, but evidence is conflicting. Utilising a national representative data of 11,714,947 pregnant women in China, we explored the immediate changes in preterm birth rates during the COVID-19 mitigation period using an interrupted-time-series analysis. We defined the period prior to February 1, 2020 as the baseline, followed by the COVID-19 mitigation stage. In the first month of the COVID-19 mitigation, a significant absolute decrease in preterm birth rates of 0.68% (95%CI:-1.10% to -0.26%) in singleton, and of 2.80% (95%CI:-4.51% to -1.09%) in multiple births was noted. This immediate decline in Wuhan was greater than that at the national level among singleton births [-2.21% (95%CI:-4.09% to -0.34% vs. -0.68%)]. Here we report an immediate impact of COVID-19 mitigation measures on preterm birth in China.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Are COVID-19 mitigation measures reducing preterm birth rate in China?BMJ Glob Health. 2021 Aug;6(8):e006359. doi: 10.1136/bmjgh-2021-006359. BMJ Glob Health. 2021. PMID: 34385161 Free PMC article.
-
Preterm birth after the introduction of COVID-19 mitigation measures in Norway, Sweden, and Denmark: a registry-based difference-in-differences study.Am J Obstet Gynecol. 2022 Apr;226(4):550.e1-550.e22. doi: 10.1016/j.ajog.2021.11.034. Epub 2021 Nov 11. Am J Obstet Gynecol. 2022. PMID: 34774824 Free PMC article.
-
Association between COVID-19 lockdown measures and the incidence of iatrogenic versus spontaneous very preterm births in the Netherlands: a retrospective study.BMC Pregnancy Childbirth. 2021 Nov 12;21(1):767. doi: 10.1186/s12884-021-04249-8. BMC Pregnancy Childbirth. 2021. PMID: 34772364 Free PMC article.
-
The impact of multiple gestations on late preterm (near-term) births.Clin Perinatol. 2006 Dec;33(4):777-92; abstract viii. doi: 10.1016/j.clp.2006.09.008. Clin Perinatol. 2006. PMID: 17148004 Review.
-
Cross-Country Individual Participant Analysis of 4.1 Million Singleton Births in 5 Countries with Very High Human Development Index Confirms Known Associations but Provides No Biologic Explanation for 2/3 of All Preterm Births.PLoS One. 2016 Sep 13;11(9):e0162506. doi: 10.1371/journal.pone.0162506. eCollection 2016. PLoS One. 2016. PMID: 27622562 Free PMC article. Review.
Cited by
-
Microbiomic insights into the unique effects of vaginal microbiota on preterm birth in Chinese pregnant women.Front Microbiol. 2025 Mar 17;16:1560528. doi: 10.3389/fmicb.2025.1560528. eCollection 2025. Front Microbiol. 2025. PMID: 40165789 Free PMC article.
-
Impact of the COVID-19 pandemic on small vulnerable newborns: an interrupted time series analysis in Peru and Brazil.J Glob Health. 2025 Jan 31;15:04026. doi: 10.7189/jogh.15.04026. J Glob Health. 2025. PMID: 39885819 Free PMC article.
-
Impact of COVID-19 pandemic on the dynamic of patients with oral and maxillofacial trauma: interrupted time-series analysis.Sci Rep. 2024 Jun 8;14(1):13202. doi: 10.1038/s41598-024-63890-3. Sci Rep. 2024. PMID: 38851787 Free PMC article.
-
Association of Ambient Air Pollution and Temperature Exposure with Placental Abruption: A Nested Case-Control Study Based on Live Birth Registrations.Environ Health Perspect. 2025 Apr;133(3-4):47013. doi: 10.1289/EHP14714. Epub 2025 Apr 29. Environ Health Perspect. 2025. PMID: 40138323 Free PMC article.
-
Reduction in spontaneous and iatrogenic preterm births in twin pregnancies during COVID-19 lockdown in Melbourne, Australia: a multicenter cohort study.BMC Pregnancy Childbirth. 2023 Dec 11;23(1):846. doi: 10.1186/s12884-023-06137-9. BMC Pregnancy Childbirth. 2023. PMID: 38082241 Free PMC article.
References
-
- WHO: recommended definitions, terminology, and format for statistical tables related to the perinatal period and use of a new certificate for cause of perinatal deaths. Modifications recommended by FIGO as amended October 14, 1976. Acta Obstet. Gynecol. Scand. 56, 247–253 (1977). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
