

A comprehensive quality assurance procedure for 4D CT commissioning and periodic QA
- PMID: 36057944
- PMCID: PMC9680562
- DOI: 10.1002/acm2.13764
A comprehensive quality assurance procedure for 4D CT commissioning and periodic QA
Abstract
Purpose: The 4D computed tomography (CT) simulation is an essential procedure for tumors exhibiting breathing-induced motion. However, to date there are no established guidelines to assess the characteristics of existing systems and to describe meaningful performance. We propose a commissioning quality assurance (QA) protocol consisting of measurements and acquisitions that assess the mechanical and computational operation for 4D CT with both phase and amplitude-based reconstructions, for regular and irregular respiratory patterns.
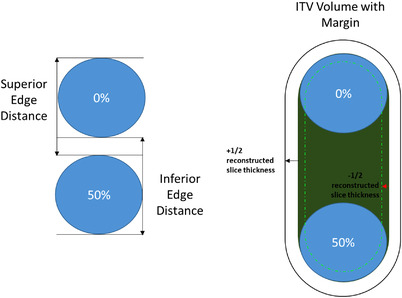
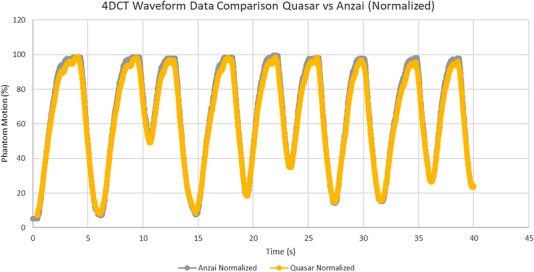
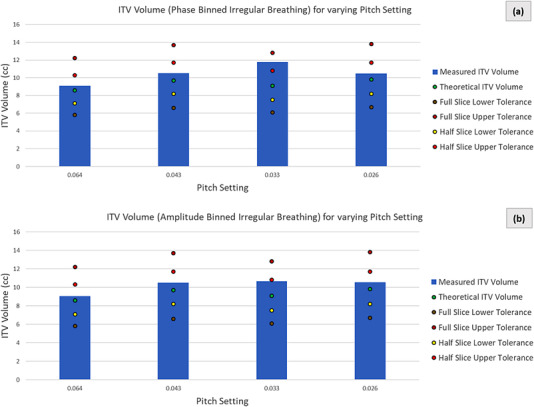
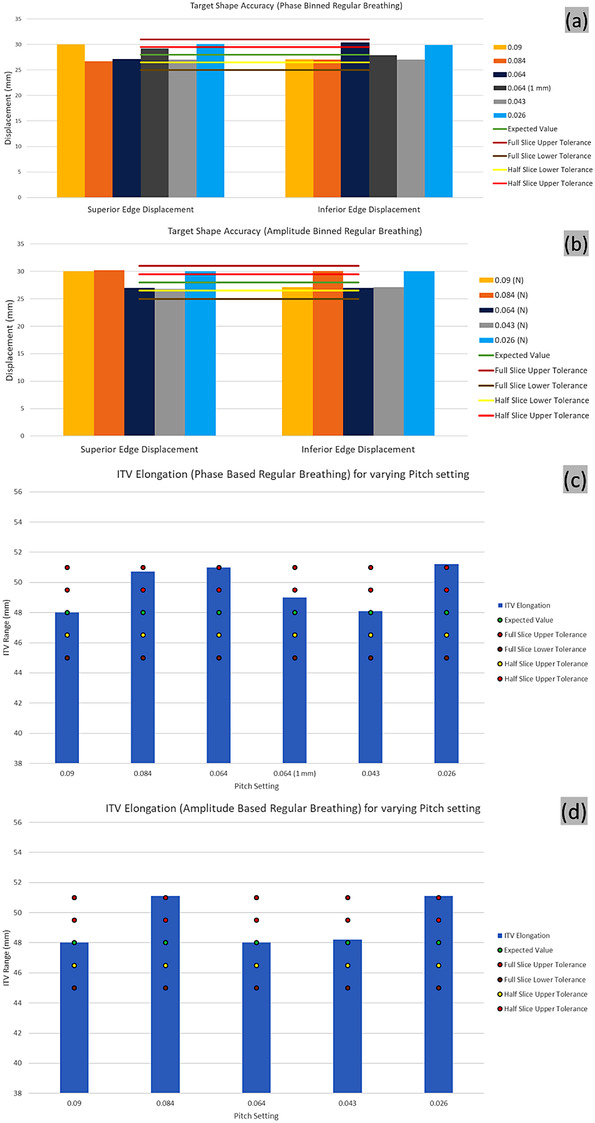
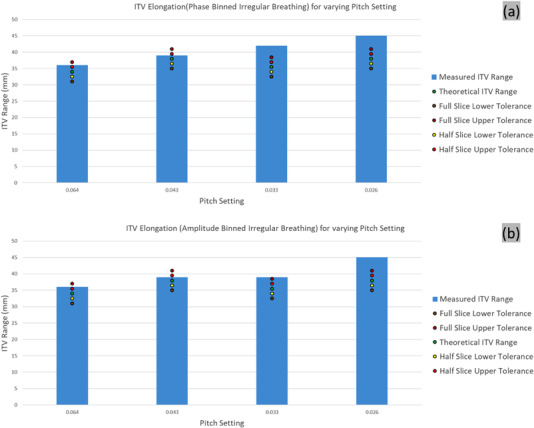
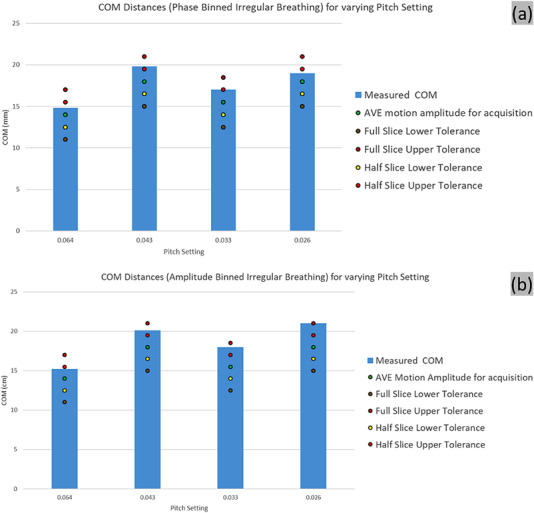
Methods: The 4D CT scans of a QUASAR motion phantom were acquired for both regular and irregular breathing patterns. The hardware consisted of the Canon Aquilion Exceed LB CT scanner used in conjunction with the Anzai laser motion monitoring system. The nominal machine performance and reconstruction were demonstrated with measurements using regular breathing patterns. For irregular breathing patterns the performance was quantified through the analysis of the target motion in the superior and inferior directions, and the volume of the internal target volume (ITV). Acquisitions were performed using multiple pitches and the reconstructions were performed using both phase and amplitude-based binning.
Results: The target was accurately captured during regular breathing. For the irregular breathing, the measured ITV exceeded the nominal ITV parameters in all scenarios, but all deviations were less than the reconstructed slice thickness. The mismatch between the nominal pitch and the actual breathing rate did not affect markedly the size of the ITV. Phase and normalized amplitude binning performed similarly.
Conclusions: We demonstrated a framework for measuring and quantifying the initial performance of 4D CT simulation scans that can also be applied during periodic QAs. The regular breathing provided confidence that the hardware and the software between the systems performs adequately. The irregular breathing data suggest that the system may be expected to capture in excess the target motion and geometry, but the deviation is expected to be within the slice thickness.
Keywords: 4D CT; CT simulation; quality assurance; radiotherapy; respiratory motion-management.
© 2022 The Authors. Journal of Applied Clinical Medical Physics published by Wiley Periodicals, LLC on behalf of The American Association of Physicists in Medicine.
Figures



References
-
- Sothmann T, Werner R, Gauer T. Influence of 4D CT motion artifacts on correspondence model‐based 4D dose accumulation. In: Webster RJ, Fei B, eds. Medical Imaging 2018: Image‐Guided Procedures, Robotic Interventions, and Modeling. 10.1117/12.2291481 - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
