Transperineal ultrasonography for treatment response evaluation in children with perianal Crohn's disease
- PMID: 36059211
- PMCID: PMC9532198
- DOI: 10.14366/usg.22057
Transperineal ultrasonography for treatment response evaluation in children with perianal Crohn's disease
Abstract
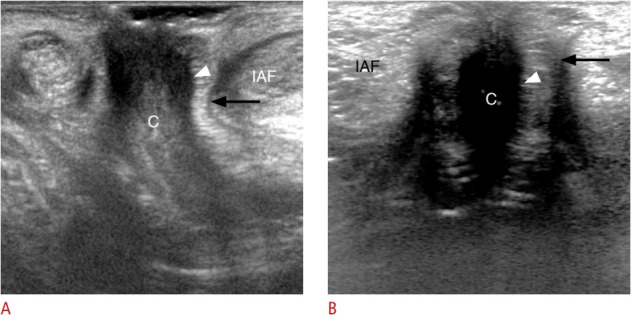
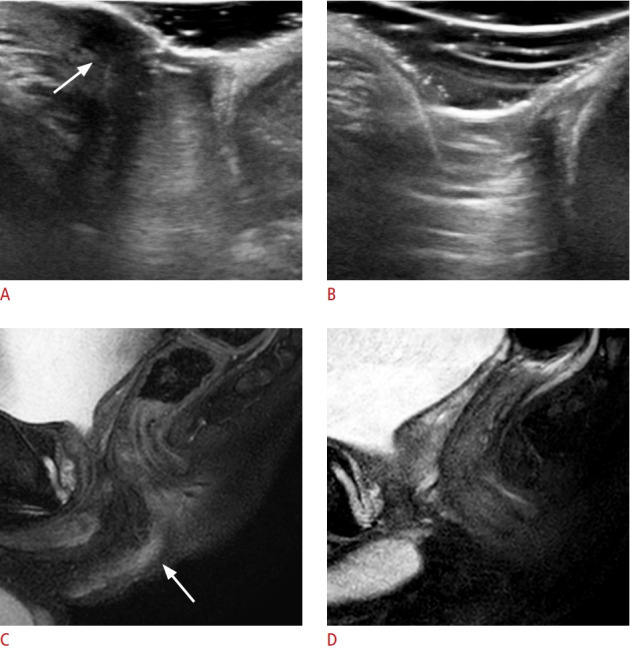
Purpose: This study assessed the performance of transperineal ultrasonography (TPUS) in evaluating the treatment response in children with perianal Crohn's disease (PACD) compared with pelvic magnetic resonance imaging (MRI).
Methods: This retrospective study was approved by the Institutional Review Board of our institution, which waived the requirement for informed consent. Twenty-nine patients (19 boys and 10 girls; median age, 14 years [range, 8 to 18 years]) with 56 fistulas were examined. Each fistula's thickness and abscess size were measured using both modalities, and treatment response was classified as positive or negative based on each modality. The concordance of the classifications was compared between TPUS and pelvic MRI. A receiver operating characteristic curve (ROC) was used to evaluate the performance of TPUS.
Results: TPUS found 80.4% (45/56) of the fistulas. On MRI, 39 fistulas (70%) were classified as having positive treatment responses, and the remaining 17 as having no response. The agreement of the classifications between TPUS and MRI was moderate (κ=0.486; P<0.001; Spearman ρ=0.573; P<0.001). Based on the ROC analysis with the MRI findings as a reference to distinguish positive from negative treatment responses, TPUS exhibited sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of 63.3%, 93.3%, 95.0%, 56.0%, and 73.3%, respectively.
Conclusion: TPUS can be an appropriate adjuvant imaging modality for pelvic MRI to evaluate the treatment response of PACD in children when initial TPUS detects PACD with a location and imaging features comparable to those visualized on MRI.
Keywords: Abscess; Anal canal; Fistula; Ultrasonography.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- de Zoeten EF, Pasternak BA, Mattei P, Kramer RE, Kader HA. Diagnosis and treatment of perianal Crohn disease: NASPGHAN clinical report and consensus statement. J Pediatr Gastroenterol Nutr. 2013;57:401–412. - PubMed
-
- Schwartz DA, Loftus EV Jr, Tremaine WJ, Panaccione R, Harmsen WS, Zinsmeister AR, et al. The natural history of fistulizing Crohn's disease in Olmsted County, Minnesota. Gastroenterology. 2002;122:875–880. - PubMed
-
- Singer AA, Gadepalli SK, Eder SJ, Adler J. Fistulizing Crohn's disease presenting after surgery on a perianal lesion. Pediatrics. 2016;137:e20152878. - PubMed
-
- Keljo DJ, Markowitz J, Langton C, Lerer T, Bousvaros A, Carvalho R, et al. Course and treatment of perianal disease in children newly diagnosed with Crohn's disease. Inflamm Bowel Dis. 2009;15:383–387. - PubMed
-
- Vernier-Massouille G, Balde M, Salleron J, Turck D, Dupas JL, Mouterde O, et al. Natural history of pediatric Crohn's disease: a population-based cohort study. Gastroenterology. 2008;135:1106–1113. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources