

Prophylactic administration of tranexamic acid combined with thromboelastography-guided hemostatic algorithm reduces allogeneic transfusion requirements during pediatric resective epilepsy surgery: A randomized controlled trial
- PMID: 36059956
- PMCID: PMC9428586
- DOI: 10.3389/fphar.2022.916017
Prophylactic administration of tranexamic acid combined with thromboelastography-guided hemostatic algorithm reduces allogeneic transfusion requirements during pediatric resective epilepsy surgery: A randomized controlled trial
Abstract
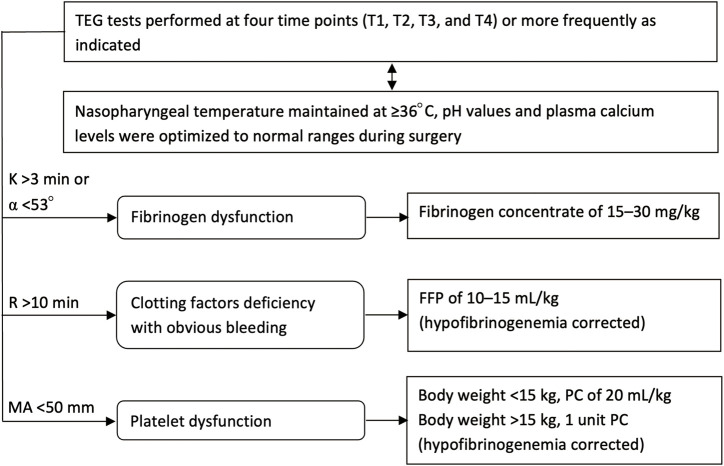
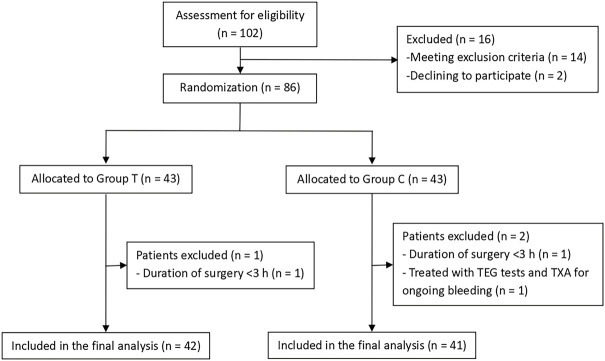
Background: Intraoperative bleeding and allogeneic transfusion remain common problems in pediatric resective epilepsy surgery. Tranexamic acid (TXA) is a widely recommended antifibrinolytic drug that reduces blood loss and transfusion requirements for bleeding patients. Thromboelastography (TEG)-guided hemostatic algorithm is commonly used in bleeding management. This trial was designed to validate the efficacy of a multimodal coagulation therapy involving continuous TXA infusion with TEG-guided hemostatic algorithm in reducing allogeneic exposure risk in pediatric resective epilepsy surgery. Methods: Eighty-three children undergoing resective epilepsy surgery were randomized into a treatment group (Group T; n = 42) and a control group (Group C; n = 41). Group T received prophylactic TXA (10 mg/kg followed by 5 mg/kg/h) with TEG-guided hemostatic algorithm, whereas Group C received conventional coagulation management. The primary outcome was allogeneic transfusion rate during surgery, and the secondary outcomes were intraoperative blood loss, incidence of postoperative seizures, and thromboembolic events during hospitalization. Results: The incidence of intraoperative allogeneic transfusion reduced by 34.7% with the use of a multimodal coagulation therapy (19.0% in Group T vs. 53.7% in Group C; RR 0.355, 95% CI 0.179-0.704; p = 0.001). This was mainly triggered by a significant reduction (44.1%) in intraoperative plasma transfusion (7.1% in Group T vs. 51.2% in Group C; RR 0.139, 95% CI 0.045-0.432; p = 0.000). The risk of intraoperative RBC transfusion was lower in Group T than in Group C, but the difference was not statistically significant (14.3% in Group T vs. 29.3% in Group C; RR 0.488, 95% CI 0.202-1.177; p = 0.098). No platelets were transfused in both groups. Further, 19 (45.2%) patients in Group T received fibrinogen concentrates guided by TEG data, whereas 1 (2.4%) patient in Group C received fibrinogen concentrates empirically. There were no significant differences in estimated blood loss and postoperative seizures between the two groups, and no thromboembolic events were observed after surgery. Conclusion: Prophylactic administration of TXA combined with TEG-guided hemostatic algorithm can be an effective multimodal coagulation strategy for reducing allogeneic transfusion requirements during pediatric resective epilepsy surgery. Clinical Trial Registration: www.chictr.org.cn/index.aspx, identifier ChiCTR1800016188.
Keywords: antifibrinolytics; blood loss; coagulation therapy; epilepsy surgery; pediatric anesthesia; thromboelastography; tranexamic acid; transfusion.
Copyright © 2022 Zhang, Feng, Xiao, Li, Liu, Feng, Qi, Fan, Shan, Yu, Zhao and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
[Influence of thromboelastography-guided hemostatic algorithm on allogeneic transfusion requirements during pediatric hemispherectomy].Zhonghua Yi Xue Za Zhi. 2024 Jun 18;104(23):2142-2147. doi: 10.3760/cma.j.cn112137-20231227-01495. Zhonghua Yi Xue Za Zhi. 2024. PMID: 38871471 Chinese.
-
Thromboelastography-guided transfusion algorithm reduces transfusions in complex cardiac surgery.Anesth Analg. 1999 Feb;88(2):312-9. doi: 10.1097/00000539-199902000-00016. Anesth Analg. 1999. PMID: 9972747 Clinical Trial.
-
Efficacy of antifibrinolytic agents on surgical bleeding and transfusion requirements in spine surgery: a meta-analysis.Eur Spine J. 2017 Jan;26(1):140-154. doi: 10.1007/s00586-016-4792-x. Epub 2016 Sep 26. Eur Spine J. 2017. PMID: 27671279 Review.
-
Prophylactic intraoperative tranexamic acid administration and postoperative blood loss after transapical aortic valve implantation.J Cardiothorac Surg. 2015 Mar 28;10:45. doi: 10.1186/s13019-015-0246-5. J Cardiothorac Surg. 2015. PMID: 25888231 Free PMC article.
-
Hemostatic effects of tranexamic acid in cardiac surgical patients with antiplatelet therapy: a systematic review and meta-analysis.Perioper Med (Lond). 2024 Jun 17;13(1):58. doi: 10.1186/s13741-024-00418-3. Perioper Med (Lond). 2024. PMID: 38886771 Free PMC article. Review.
Cited by
-
The effect of triple-dose-intravenous tranexamic acid on blood loss in patients undergoing total hip arthroplasty without affecting blood coagulopathy: A prospective thromboelastographic analysis.Acta Orthop Traumatol Turc. 2023 Nov 21;57(6):378-83. doi: 10.5152/j.aott.2023.23001. Online ahead of print. Acta Orthop Traumatol Turc. 2023. PMID: 37987599 Free PMC article.
-
The efficacy and safety of topical combined with intravenous administration of tranexamic acid in spine surgery: a systematic review and meta-analysis.BMC Musculoskelet Disord. 2024 Dec 27;25(1):1074. doi: 10.1186/s12891-024-08191-6. BMC Musculoskelet Disord. 2024. PMID: 39725950 Free PMC article.
References
-
- Dadure C., Sauter M., Bringuier S., Bigorre M., Raux O., Rochette A., et al. (2011). Intraoperative tranexamic acid reduces blood transfusion in children undergoing craniosynostosis surgery: A randomized double-blind study. Anesthesiology 114 (4), 856–861. 10.1097/ALN.0b013e318210f9e3 - DOI - PubMed
LinkOut - more resources
Full Text Sources