

Fetal growth restriction and stillbirth: Biomarkers for identifying at risk fetuses
- PMID: 36060697
- PMCID: PMC9437293
- DOI: 10.3389/fphys.2022.959750
Fetal growth restriction and stillbirth: Biomarkers for identifying at risk fetuses
Abstract
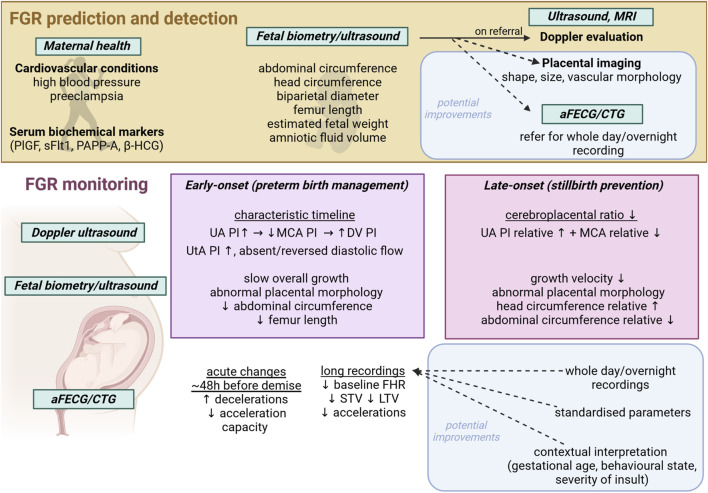
Fetal growth restriction (FGR) is a major cause of stillbirth, prematurity and impaired neurodevelopment. Its etiology is multifactorial, but many cases are related to impaired placental development and dysfunction, with reduced nutrient and oxygen supply. The fetus has a remarkable ability to respond to hypoxic challenges and mounts protective adaptations to match growth to reduced nutrient availability. However, with progressive placental dysfunction, chronic hypoxia may progress to a level where fetus can no longer adapt, or there may be superimposed acute hypoxic events. Improving detection and effective monitoring of progression is critical for the management of complicated pregnancies to balance the risk of worsening fetal oxygen deprivation in utero, against the consequences of iatrogenic preterm birth. Current surveillance modalities include frequent fetal Doppler ultrasound, and fetal heart rate monitoring. However, nearly half of FGR cases are not detected in utero, and conventional surveillance does not prevent a high proportion of stillbirths. We review diagnostic challenges and limitations in current screening and monitoring practices and discuss potential ways to better identify FGR, and, critically, to identify the "tipping point" when a chronically hypoxic fetus is at risk of progressive acidosis and stillbirth.
Keywords: biomarkers; fetal growth restriction (FGR); fetal heart rate variability (fHRV); fetal hypoxia; preterm brain injury; stillbirth.
Copyright © 2022 King, Bennet, Stone, Clark, Gunn and Dhillon.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Amorim-Costa C., de Campos D. A., Bernardes J. (2017a). Cardiotocographic parameters in small-for-gestational-age fetuses: How do they vary from normal at different gestational ages? A study of 11687 fetuses from 25 to 40 weeks of pregnancy. J. Obstet. Gynaecol. Res. 43 (3), 476–485. 10.1111/jog.13235 - DOI - PubMed
-
- Amorim-Costa C., Gaio A. R., Ayres-de-Campos D., Bernardes J. (2017b). Longitudinal changes of cardiotocographic parameters throughout pregnancy: A prospective cohort study comparing small-for-gestational-age and normal fetuses from 24 to 40 weeks. J. Perinat. Med. 45 (4), 493–501. 10.1515/jpm-2016-0065 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous