

Acute piriformis syndrome mimicking cauda equina syndrome: illustrative case
- PMID: 36060900
- PMCID: PMC9435562
- DOI: 10.3171/CASE21252
Acute piriformis syndrome mimicking cauda equina syndrome: illustrative case
Abstract
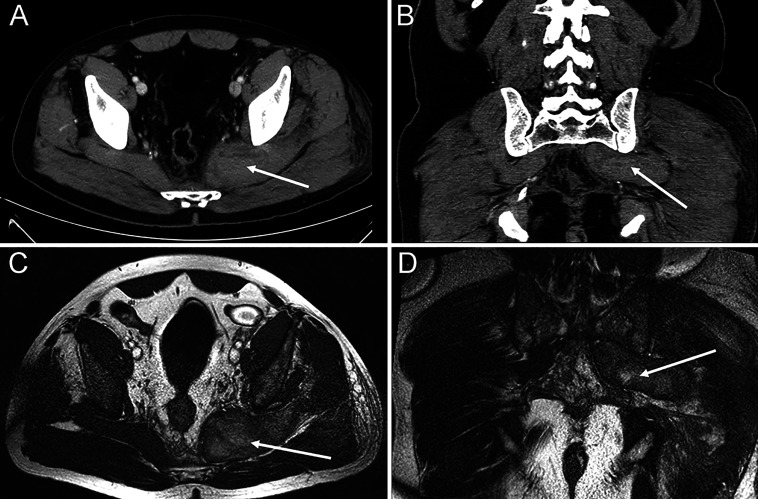
Background: This report depicts a rare case of acutely developed urinary retention as well as sensory and motor disturbances caused by formation of a large hematoma within the piriformis muscle, which caused compression of nerves within the suprapiriform and infrapiriform foramina, thus imitating cauda equina syndrome. Although cases of acute lumbosacral plexopathy have been described, this case is the first time both urinary retention and sensory and motor disturbances were present.
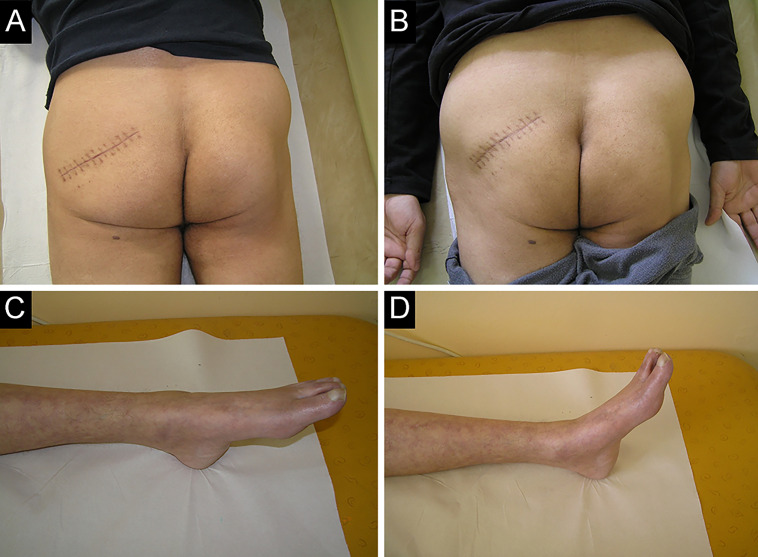
Observations: The most useful tools for diagnosis of acute piriformis syndrome are detailed patient history, magnetic resonance imaging (MRI) of the pelvic region, and electrophysiological testing performed by an experienced electrophysiologist. As a result of diligent rehabilitation, including physiotherapy and electrostimulation, the patient was able to successfully recover, regardless of acute compression of the sacral plexus that lasted 6 days.
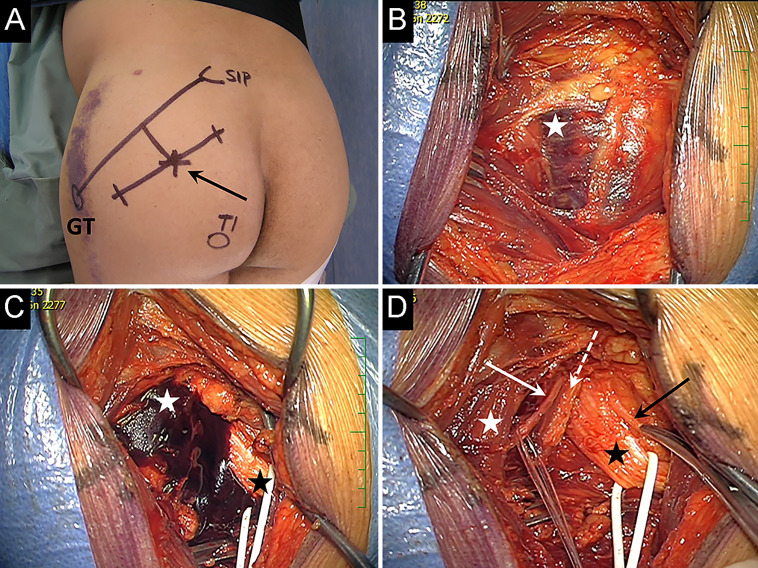
Lessons: Clinicians should actively ask about previous pelvic trauma when taking a patient history in similar cases, especially if the patient is receiving anticoagulation treatment. If MRI of the lumbar spine does not reveal any pathologies, MRI of the pelvic region should be performed. Acute surgical decompression is crucial for preserving neurological function. In similar cases, it is possible to differentiate between spinal cord, cauda equina, and pelvic lesions using electrophysiological studies.
Keywords: CES = cauda equina syndrome; CMCT = central motor conduction time; CT = computed tomography; EMG = electromyography; LSP = lumbosacral plexopathy; MRI = magnetic resonance imaging; PS = piriformis syndrome; cauda equina; lumbosacral plexus; piriformis syndrome; urinary retention.
© 2021 The authors.
Conflict of interest statement
Disclosures The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Figures
Similar articles
-
Piriformis syndrome as a result of intramuscular haematoma mimicking cauda equina effectively treated with piriformis tendon release.BMJ Case Rep. 2022 Mar 2;15(3):e247988. doi: 10.1136/bcr-2021-247988. BMJ Case Rep. 2022. PMID: 35236695 Free PMC article.
-
Clinical Presentation and Physiotherapy Rehabilitation of Cauda Equina Syndrome with Urinary Incontinence: A Case Report.Cureus. 2024 Sep 26;16(9):e70236. doi: 10.7759/cureus.70236. eCollection 2024 Sep. Cureus. 2024. PMID: 39463676 Free PMC article.
-
Does a history of lumbar spine surgery predict radiological cauda equina compression in patients undergoing MRI for suspected cauda equina syndrome?Br J Neurosurg. 2020 Feb;34(1):76-79. doi: 10.1080/02688697.2019.1687845. Epub 2019 Nov 13. Br J Neurosurg. 2020. PMID: 31718292
-
Differential diagnosis and treatment of acute cauda equina syndrome in the human immunodeficiency virus positive patient: a case report and review of the literature.J Med Case Rep. 2016 Jun 6;10:165. doi: 10.1186/s13256-016-0902-y. J Med Case Rep. 2016. PMID: 27268102 Free PMC article. Review.
-
Cauda equina, conus medullaris and syndromes mimicking sciatic pain: WFNS spine committee recommendations.World Neurosurg X. 2024 Feb 10;22:100274. doi: 10.1016/j.wnsx.2024.100274. eCollection 2024 Apr. World Neurosurg X. 2024. PMID: 38496349 Free PMC article. Review.
Cited by
-
Atypical lipoma of the right piriformis muscle: a case report and review of the literature.J Med Case Rep. 2024 Mar 31;18(1):189. doi: 10.1186/s13256-024-04507-1. J Med Case Rep. 2024. PMID: 38555435 Free PMC article. Review.
-
Piriformis syndrome as a result of intramuscular haematoma mimicking cauda equina effectively treated with piriformis tendon release.BMJ Case Rep. 2022 Mar 2;15(3):e247988. doi: 10.1136/bcr-2021-247988. BMJ Case Rep. 2022. PMID: 35236695 Free PMC article.
References
-
- Stranding S. Gray’s Anatomy: The Anatomical Basis of Clinical Practice. 42nd ed. Elsevier; 2020.
-
- Parlak A, Aytekin A, Develi S, Ekinci S. Piriformis syndrome: a case with non-discogenic sciatalgia. Turk Neurosurg. 2014;24(1):117–119. - PubMed
-
- Dydyk AM, Hameed S. Lumbosacral Plexopathy. StatPearls; 2021. - PubMed
-
- Dyck PJ, Thaisetthawatkul P. Lumbosacral plexopathy. Continuum (Minneap Minn) 2014;20(5 Peripheral Nervous System Disorders):1343–1358. - PubMed
-
- Planner AC, Donaghy M, Moore NR. Causes of lumbosacral plexopathy. Clin Radiol. 2006;61(12):987–995. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
