

Application of modified subtotal resection of adenomyosis combined with LNG-IUS and GnRH-a sequential therapy in severe adenomyosis: A case series
- PMID: 36061067
- PMCID: PMC9434309
- DOI: 10.3389/fsurg.2022.914725
Application of modified subtotal resection of adenomyosis combined with LNG-IUS and GnRH-a sequential therapy in severe adenomyosis: A case series
Abstract
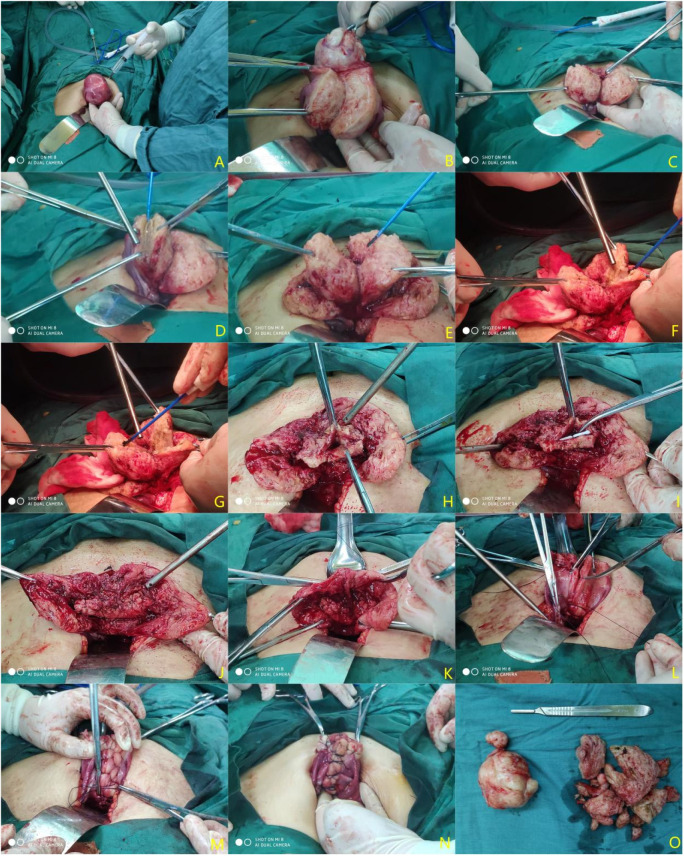
Background and objective: Adenomyosis focus resection has always been the main surgical method for patients with uterine preservation, but its curative effect and surgical method are still controversial. We improved this method on the basis of the "double-flap method" and combined it with the levonorgestrel intrauterine delivery system (LNG-IUS) and gonadotropin-releasing hormone agonist (GnRH-a) sequential treatment to determine the clinical effect and feasibility of this scheme in the treatment of severe adenomyosis.
Methods: This is a retrospective review. A total of 64 patients with severe adenomyosis were treated in the Department of Gynecology of Changzhou Second People's Hospital, which is affiliated to Nanjing Medical University, from December 2017 to September 2021. The transabdominal approach and laparoscopic approach were adopted for the purposes of treatment in this study. Hence, the patients were subdivided into the transabdominal approach subgroup and the laparoscopic approach subgroup. The hemoglobin, visual analog score (VAS) score, menstruation score, and other indices of each patient before and after treatment were observed, recorded, and analyzed.
Results: All 64 patients underwent the operation successfully. After the completion of sequential treatment, the CA125 decreased significantly 1 month after the operation, the average uterine volume significantly reduced, the hemoglobin value increased to a certain extent 3 months after the operation, and the menstrual score and dysmenorrhea during the first menstruation were significantly lower than they were before the operation. After the treatment, the therapeutic results of the transabdominal approach subgroup and endoscopic approach subgroup were compared on the basis of the observed indices, and no significant difference was observed (P > 0.05). Only one patient had a downward movement of the LNG-IUS, and the vaginal ultrasound showed that the upper end of the LNG-IUS was approximately 1.5 cm from the bottom of the uterine cavity. The average follow-up period was 24.02 ± 11.77 months, and no lesion progression was found in any patients.
Conclusion: For patients suffering from severe adenomyosis who have no pregnancy plans and require uterine preservation, transabdominal or laparoscopic subtotal resection of the focus of adenomyosis, combined with the LNG-IUS + GnRH-a sequential treatment, may be a safe and effective alternative when conservative treatments such as drugs fail.
Keywords: dysmenorrhea; gonadotropin-releasing hormone agonist; levonorgestrel intrauterine delivery system; severe adenomyosis; subtotal resection of adenomyosis.
© 2022 Qin, Dong, Tang, Zhang, Wang, Bao, Wei, Shi, Chen and Xia.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Combined therapeutic effects of HIFU, GnRH-a and LNG-IUS for the treatment of severe adenomyosis.Int J Hyperthermia. 2019;36(1):486-492. doi: 10.1080/02656736.2019.1595179. Epub 2019 Apr 17. Int J Hyperthermia. 2019. PMID: 30994010
-
Clinical evaluation of high-intensity focused ultrasound ablation combined with mifepristone and levonorgestrel-releasing intrauterine system to treat symptomatic adenomyosis.Int J Hyperthermia. 2023;40(1):2161641. doi: 10.1080/02656736.2022.2161641. Int J Hyperthermia. 2023. PMID: 36586419
-
Treatment of symptomatic adenomyosis with the levonorgestrel-releasing intrauterine system.Int J Gynaecol Obstet. 2019 Sep;146(3):357-363. doi: 10.1002/ijgo.12887. Epub 2019 Jun 27. Int J Gynaecol Obstet. 2019. PMID: 31194884
-
Long-term efficacy and safety of levonorgestrel releasing intrauterine system in the treatment of adenomyosis: evidence mapping.Arch Gynecol Obstet. 2024 Jul;310(1):55-67. doi: 10.1007/s00404-024-07546-7. Epub 2024 Jun 5. Arch Gynecol Obstet. 2024. PMID: 38836931 Review.
-
Effectiveness of high-intensity focused ultrasound combined with gonadotropin-releasing hormone agonist or combined with levonorgestrel-releasing intrauterine system for adenomyosis: A systematic review and meta-analysis.Taiwan J Obstet Gynecol. 2024 Jul;63(4):492-499. doi: 10.1016/j.tjog.2024.01.036. Taiwan J Obstet Gynecol. 2024. PMID: 39004475
Cited by
-
Individualized conservative therapeutic strategies for adenomyosis with the aim of preserving fertility.Front Med (Lausanne). 2023 Mar 30;10:1133042. doi: 10.3389/fmed.2023.1133042. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37064035 Free PMC article. Review.
-
Effects of different treatment methods on clinical efficacy and fertility outcomes of patients with adenomyosis.J Ovarian Res. 2024 Jan 12;17(1):16. doi: 10.1186/s13048-023-01320-0. J Ovarian Res. 2024. PMID: 38216945 Free PMC article.
References
-
- Graziano A, Lo Monte G, Piva I, Caserta D, Karner M, Engl B, et al. Diagnostic findings in adenomyosis: a pictorial review on the major concerns. Eur Rev Med Pharmacol Sci. (2015) 19(7):1146–54. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous