

Clinical Phenotypes of Heart Failure With Preserved Ejection Fraction to Select Preclinical Animal Models
- PMID: 36061340
- PMCID: PMC9436760
- DOI: 10.1016/j.jacbts.2021.12.009
Clinical Phenotypes of Heart Failure With Preserved Ejection Fraction to Select Preclinical Animal Models
Abstract
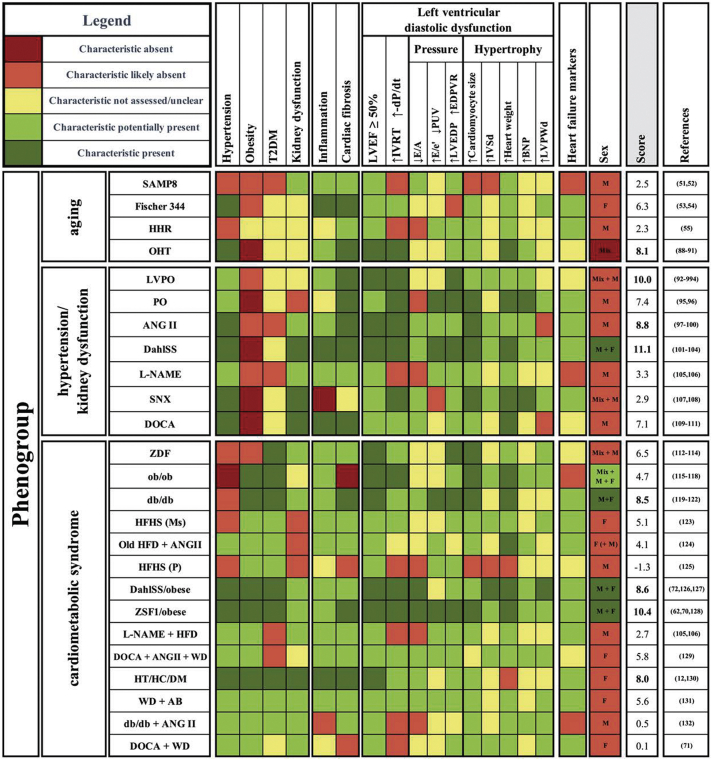
At least one-half of the growing heart failure population consists of heart failure with preserved ejection fraction (HFpEF). The limited therapeutic options, the complexity of the syndrome, and many related comorbidities emphasize the need for adequate experimental animal models to study the etiology of HFpEF, as well as its comorbidities and pathophysiological changes. The strengths and weaknesses of available animal models have been reviewed extensively with the general consensus that a "1-size-fits-all" model does not exist, because no uniform HFpEF patient exists. In fact, HFpEF patients have been categorized into HFpEF phenogroups based on comorbidities and symptoms. In this review, we therefore study which animal model is best suited to study the different phenogroups-to improve model selection and refinement of animal research. Based on the published data, we extrapolated human HFpEF phenogroups into 3 animal phenogroups (containing small and large animals) based on reports and definitions of the authors: animal models with high (cardiac) age (phenogroup aging); animal models focusing on hypertension and kidney dysfunction (phenogroup hypertension/kidney failure); and models with hypertension, obesity, and type 2 diabetes mellitus (phenogroup cardiometabolic syndrome). We subsequently evaluated characteristics of HFpEF, such as left ventricular diastolic dysfunction parameters, systemic inflammation, cardiac fibrosis, and sex-specificity in the different models. Finally, we scored these parameters concluded how to best apply these models. Based on our findings, we propose an easy-to-use classification for future animal research based on clinical phenogroups of interest.
Keywords: ANGII, angiotensin II; BNP, brain natriuretic peptide; DOCA, deoxycorticosterone acetate; DahlSS, Dahl salt sensitive; HF, heart failure; HFD, high-fat diet; HFHS, high fat, high sugar; HFpEF; HFpEF, heart failure with preserved ejection fraction; HHR, hypertrophic heart rat; IVRT, isovolumetric relaxation time; L-NAME, Nω-nitrol-arginine methyl ester; LV, left ventricle/ventricular; LVDD; LVDD, left ventricular diastolic dysfunction; LVEDP, left ventricular end-diastolic pressure; LVEF, left ventricular ejection fraction; PO, pressure overload; T2DM, type 2 diabetes mellitus; ZSF1, Zucker fatty and spontaneously hypertensive; animal models; heart failure with preserved ejection fraction; left ventricular diastolic dysfunction; phenogroups.
© 2022 The Authors.
Conflict of interest statement
This work was supported by Netherlands Cardiovascular Research Initiative, with the support of the Dutch Heart Foundation, the Netherlands (CVON2018-30 PREDICT2 to Drs van Ham and van Veen, Senior Clinical Scientist grant 2020T058 to Dr Handoko; EARLY-HFpEF Young Talent Grant 2015-10 to Dr Kessler, RECONNEXT 2020B008 and IMPRESS 2020B004 to Drs Kessler, Handoko, den Ruijter, and de Jager). The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures



References
-
- Pandey A., Patel K., Vaduganathan M., et al. Physical activity, fitness, and obesity in heart failure with preserved ejection fraction. J Am Coll Cardiol HF. 2018;6(12):975–982. - PubMed
-
- Streng K., Nauta J., Hillege H., et al. Non-cardiac comorbidities in heart failure with reduced, mid-range and preserved ejection fraction. Int J Cardiol. 2018;271:132–139. - PubMed
-
- Tibrewala A., Yancy C. Heart failure with preserved ejection fraction in women. Heart Fail Clin. 2019;15(1):9–18. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
