

Arthroscopic Modified McLaughlin Procedure and Remplissage for Treatment of Simultaneous Reverse Hill-Sachs and Hill-Sachs Lesions
- PMID: 36061462
- PMCID: PMC9437510
- DOI: 10.1016/j.eats.2022.03.038
Arthroscopic Modified McLaughlin Procedure and Remplissage for Treatment of Simultaneous Reverse Hill-Sachs and Hill-Sachs Lesions
Abstract
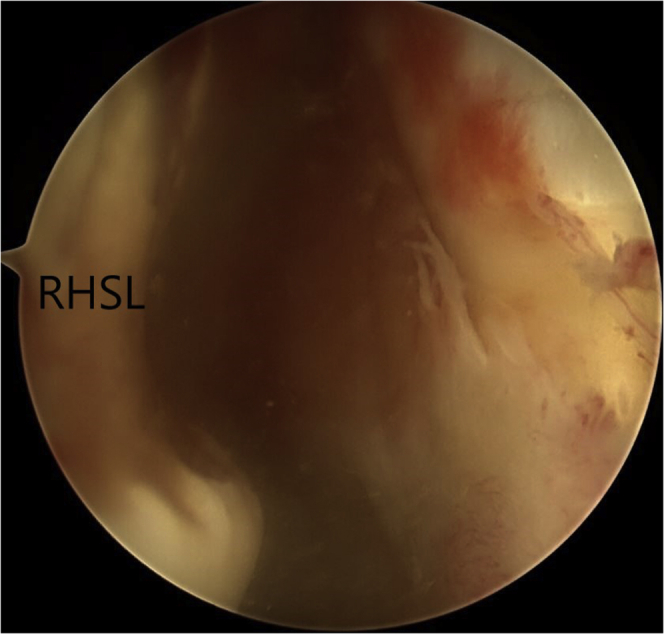
Hill-Sachs lesions (HSLs) can be present after a primary shoulder dislocation and may go unrecognized; this can alter the necessary bony constraint within the glenohumeral joint. To deal with HSLs, remplissage is a safe procedure with low complication rates, low recurrent instability rates, and good patient outcome scores compared with many of the other alternative techniques. On the other hand, a great number of techniques have been described to treat reverse Hill-Sachs lesions (RHSLs). In this article, we propose a method of treatment for combined simultaneous HSL and RHSL shoulder injuries. However, consensus on a specific treatment is yet to be established. We present an arthroscopic treatment guideline for patients with shoulder instability due to anterior and posterior labral lesions, HSL, and RHSL.
© 2022 The Authors.
Figures








References
-
- Haley C.C.A. History and physical examination for shoulder instability. Sports Med Arthrosc Rev. 2017;25:150–155. - PubMed
-
- Coyner K.J., Arciero R.A. Shoulder instability: Anterior, posterior, multidirectional, arthroscopic versus open, bone block procedures. Sports Med Arthrosc Rev. 2018;26:168–170. - PubMed
LinkOut - more resources
Full Text Sources
