

Sleep apnea predicts cardiovascular death in patients with Marfan syndrome: a cohort study
- PMID: 36061830
- PMCID: PMC9437159
- DOI: 10.1007/s13167-022-00291-4
Sleep apnea predicts cardiovascular death in patients with Marfan syndrome: a cohort study
Abstract
Background: Surgical replacement of the aortic root is the only intervention that can prevent aortic dissection and cardiovascular death in Marfan syndrome (MFS). However, in some individuals, MFS also causes sleep apnea. If sleep apnea predicts cardiovascular death, a new target for predictive, preventive, and personalized medicine (PPPM) may emerge for those individuals with MFS who have sleep apnea.
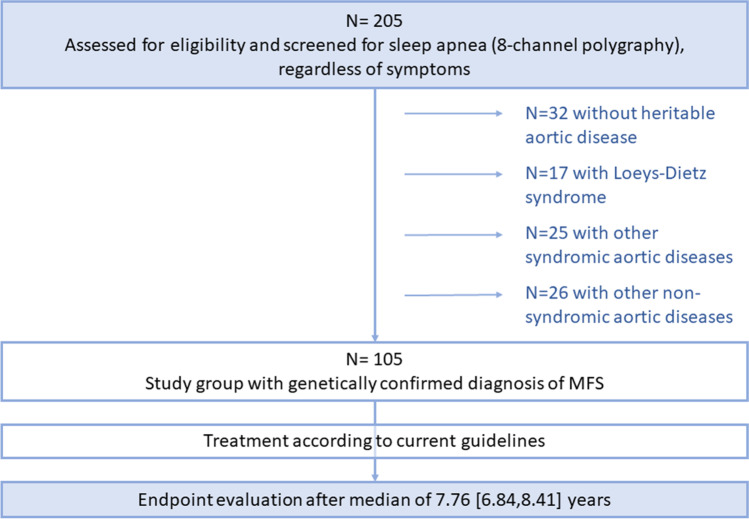
Methods: This is an investigator-initiated study with long-term follow-up data of 105 individuals with MFS. All individuals were screened for sleep apnea regardless of symptoms. Cardiovascular death served as a primary endpoint, and aortic events as a secondary outcome.
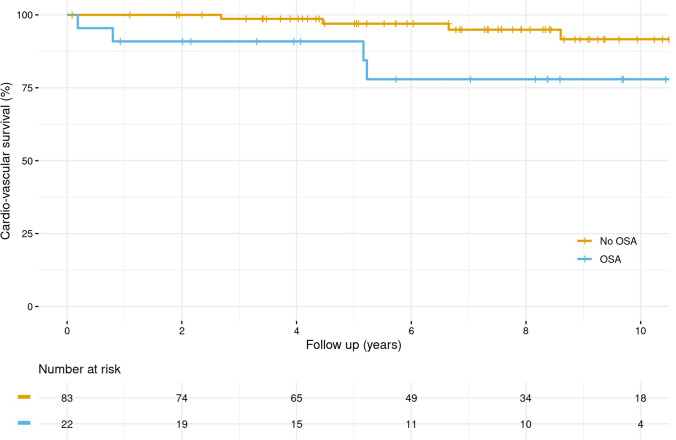
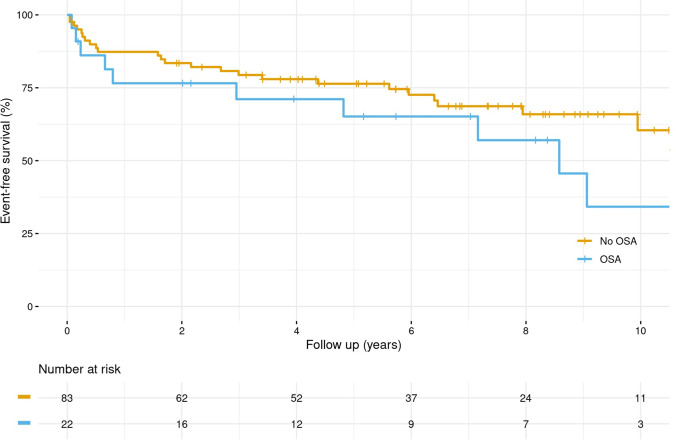
Results: Sleep apnea with an apnea-hypopnea index (AHI) > 5/h was observed in 21.0% (22/105) with mild sleep apnea in 13% (14/105) and moderate to severe sleep apnea in 7.6% (8/105). After a median follow-up of 7.76 years (interquartile range: 6.84, 8.41), 10% (10/105) had died, with cardiovascular cause of death in 80% (8/10). After adjusting for age and body mass index (BMI), the AHI score emerged as an independent risk factor for cardiovascular death (hazard ratio 1.712, 95% confidence interval [1.061-2.761], p = 0.0276). The secondary outcome of aortic events occurred in 33% (35/105). There was no effect of the AHI score on aortic events after adjusting for age and BMI (hazard ratio 0.965, 95% confidence interval [0.617-1.509]), possibly due to a high number of patients with prior aortic surgery.
Interpretation: Sleep apnea is emerging as an independent predictor of cardiovascular death in MFS. It seems mandatory to screen all individuals with MFS for sleep apnea and to include these individuals, with both MFS and sleep apnea, in further studies to evaluate the impact of preventive measures with regard to cardiovascular death.
Supplementary information: The online version contains supplementary material available at 10.1007/s13167-022-00291-4.
Keywords: Aortic rupture; Cardiovascular death; Connective tissue deficits; Marfan syndrome; Mortality; Predictive preventive personalized medicine; Sleep apnea.
© The Author(s) 2022.
Conflict of interest statement
Competing interestsNG reports grants from Boston Scientific, grants from Medtronic, and support from Bayer Vital, outside the submitted work. SD reports institutional grants from COOK Medical and honoraria from Bayer Vital, outside the submitted work. CE reports grants and/or personal fees from Abbott, Biosense Webster, Biotronik, Boehringer Ingelheim, Boston Scientific, Bristol Myers Squibb, Daiichi Sankyo and Medtronic, outside the submitted work. SH reports grants from Meril Life, Boston Scientific and Spectranetics, outside the submitted work. ET reports honoraria from Abiomed and travel compensation from Bayer Vital, Edwards, and Amgen, outside the submitted work. SW reports grants and personal fees from Abbott, Boston Scientific, and Medtronic, and personal feels from Abbott, Boehringer Ingelheim, Bristol Myers Squibb, Bayer Vital, Acutus, and Daiichi Sankyo, outside the submitted work. All other authors have nothing to disclose.
Figures
References
-
- von Kodolitsch Y, De Backer J, Schüler H, Bannas P, Behzadi C, Bernhardt AM, Hillebrand M, Fuisting B, Sheikhzadeh S, Rybczynski M, Kölbel T, Püschel K, Blankenberg S, Robinson PN. Perspectives on the revised Ghent criteria for the diagnosis of Marfan syndrome. Appl Clin Genet. 2015;16(8):137–155. doi: 10.2147/TACG.S60472. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
