

Successful Treatment of Intracranial Methotrexate-associated Lymphoproliferative Disorder without Epstein-Barr Virus Infection Using Rituximab, Methotrexate, Procarbazine, and Vincristine: A Case Report
- PMID: 36061907
- PMCID: PMC9398467
- DOI: 10.2176/jns-nmc.2022-0091
Successful Treatment of Intracranial Methotrexate-associated Lymphoproliferative Disorder without Epstein-Barr Virus Infection Using Rituximab, Methotrexate, Procarbazine, and Vincristine: A Case Report
Abstract
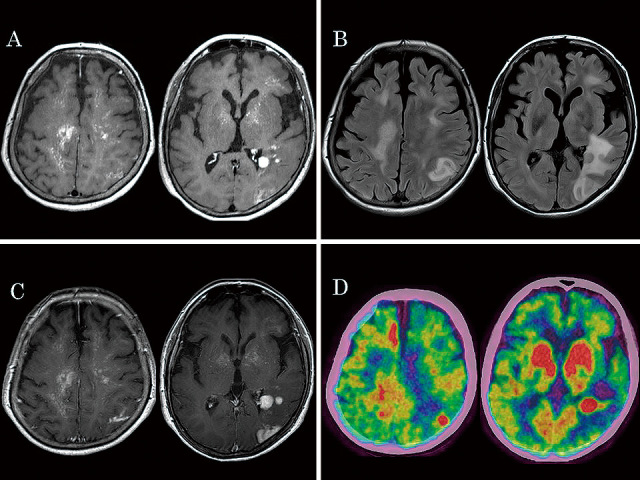
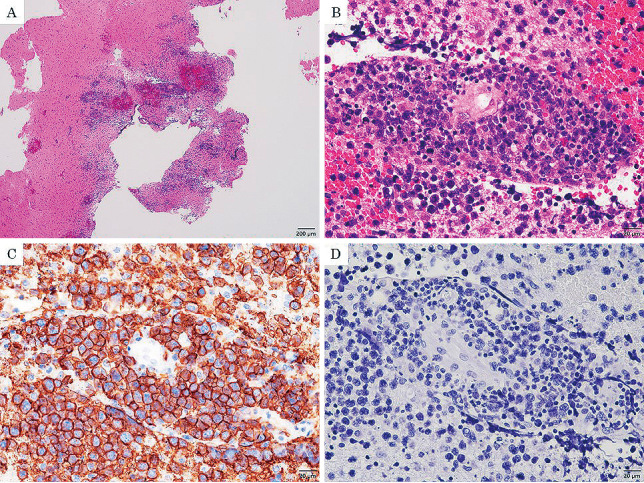
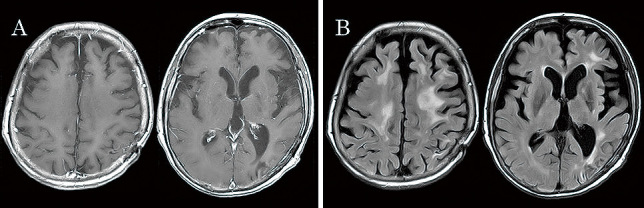
Methotrexate-associated lymphoproliferative disorder (MTX-LPD) occurs in patients with rheumatoid arthritis (RA) treated with methotrexate (MTX). MTX-LPD is typically associated with Epstein-Barr virus (EBV) infection and regresses with MTX discontinuation. On the other hand, EBV-negative MTX-LPDs are less common and are more likely to show partial or no regression after MTX discontinuation. There were no standard chemotherapeutic options for refractory MTX-LPD. We present a case of EBV-negative MTX-LPD in the central nervous system (CNS) that was successfully treated with rituximab, methotrexate, procarbazine, and vincristine (R-MPV), followed by reduced-dose whole-brain radiotherapy (rdWBRT), following the same treatment protocol as primary CNS lymphoma. A 59-year-old woman with RA treated with MTX presented with gradually developing staggered gait, memory deficit, and disorientation. Multiple lesions with heterogeneous contrast enhancement were discovered using brain magnetic resonance imaging. The patient was suspected of having MTX-LPD, but discontinuing MTX did not result in regression of the brain lesions. She underwent a biopsy from the left parietal lesion. The tissue was pathologically diagnosed as diffuse large B-cell lymphoma. Furthermore, pathological examination through EBV-encoded ribonucleic acid in situ hybridization demonstrated a lack of EBV infection. She was ultimately diagnosed with EBV-negative CNS MTX-LPD. We applied chemotherapy with R-MPV and rdWBRT. The patient achieved a complete response. In the case of CNS MTX-LPD without EBV infection, chemotherapy with R-MPV followed by rdWBRT may be considered.
Keywords: methotrexate; methotrexate-associated lymphoproliferative disorder (MTX-LPD); primary central nervous system lymphoma (PCNSL); rheumatoid arthritis; rituximab, methotrexate, procarbazine, and vincristine (R-MPV).
© 2022 The Japan Neurosurgical Society.
Conflict of interest statement
All authors have no conflict of interest.
Figures
Similar articles
-
Spontaneous regression of breast lymphoproliferative disorders after withdrawal of methotrexate in rheumatoid arthritis patients with Epstein-Barr virus infection: a case report and review of the literature.J Med Case Rep. 2022 Feb 7;16(1):49. doi: 10.1186/s13256-022-03274-1. J Med Case Rep. 2022. PMID: 35125110 Free PMC article. Review.
-
Cessation of methotrexate and a small intestinal resection provide a good clinical course for a patient with a jejunum perforation induced by a methotrexate-associated lymphoproliferative disorder: a case report.World J Surg Oncol. 2021 Jan 2;19(1):4. doi: 10.1186/s12957-020-02114-0. World J Surg Oncol. 2021. PMID: 33388058 Free PMC article.
-
Primary Central Nervous System Methotrexate-associated Lymphoproliferative Disorder in a Patient with Rheumatoid Arthritis: Case Report and Review of Literature.NMC Case Rep J. 2020 Jun 26;7(3):121-127. doi: 10.2176/nmccrj.cr.2019-0241. eCollection 2020 Jul. NMC Case Rep J. 2020. PMID: 32695560 Free PMC article.
-
Methotrexate-related Epstein-Barr virus-associated lymphoproliferative disorder occurring in the gingiva of a patient with rheumatoid arthritis.Int J Clin Exp Pathol. 2013 Sep 15;6(10):2237-41. eCollection 2013. Int J Clin Exp Pathol. 2013. PMID: 24133604 Free PMC article.
-
Epstein-Barr virus-related lymphoma in rheumatoid arthritis: implications for long-term usage of immunosuppressive drugs and review of the literature.Intern Med J. 2022 Oct;52(10):1717-1723. doi: 10.1111/imj.15390. Epub 2022 May 23. Intern Med J. 2022. PMID: 34028145 Review.
Cited by
-
Extranodal lymphoma: pathogenesis, diagnosis and treatment.Mol Biomed. 2023 Sep 18;4(1):29. doi: 10.1186/s43556-023-00141-3. Mol Biomed. 2023. PMID: 37718386 Free PMC article. Review.
-
Methotrexate‑related other iatrogenic immunodeficiency‑associated lymphoproliferative disorder in the CNS and medication‑related osteonecrosis of the jaw occurring simultaneously: A case report.Exp Ther Med. 2023 Nov 28;27(1):41. doi: 10.3892/etm.2023.12329. eCollection 2024 Jan. Exp Ther Med. 2023. PMID: 38125353 Free PMC article.
-
Lymphoproliferative disorder during temozolomide therapy; a representative case of a formidable complication and management challenges.BMC Neurol. 2023 Jun 9;23(1):224. doi: 10.1186/s12883-023-03274-8. BMC Neurol. 2023. PMID: 37296412 Free PMC article.
References
-
- Shiroky JB, Frost A, Skelton JD, Haegert DG, Newkirk MM, Neville C: Complications of immunosuppression associated with weekly low dose methotrexate. J Rheumatol 18: 1172-1175, 1991 - PubMed
-
- Wolfe F, Michaud K: The effect of methotrexate and anti-tumor necrosis factor therapy on the risk of lymphoma in rheumatoid arthritis in 19,562 patients during 89,710 person-years of observation. Arthritis Rheum 56: 1433-1439, 2007 - PubMed
-
- Hoshida Y, Xu JX, Fujita S, et al. : Lymphoproliferative disorders in rheumatoid arthritis: Clinicopathological analysis of 76 cases in relation to methotrexate medication. J Rheumatol 34: 322-331, 2007 - PubMed
-
- Kikuchi J, Kaneko Y, Kasahara H, et al. : Methotrexate-associated intravascular large B-cell lymphoma in a patient with rheumatoid arthritis. Intern Med 55: 1661-1665, 2016 - PubMed
-
- Uchida Y, Hokkoku K, Hatanaka Y, Kikuchi Y, Tashiro H, Sonoo M: Primary central nervous system methotrexate associated lymphoproliferative disorders in a patient with rheumatoid arthritis. Rinsho Shinkeigaku 58: 485-491, 2018 - PubMed
Publication types
LinkOut - more resources
Full Text Sources