

Percutaneous Chest Tube for Pleural Effusion and Pneumothorax
- PMID: 36062227
- PMCID: PMC9433150
- DOI: 10.1055/s-0042-1751295
Percutaneous Chest Tube for Pleural Effusion and Pneumothorax
Abstract
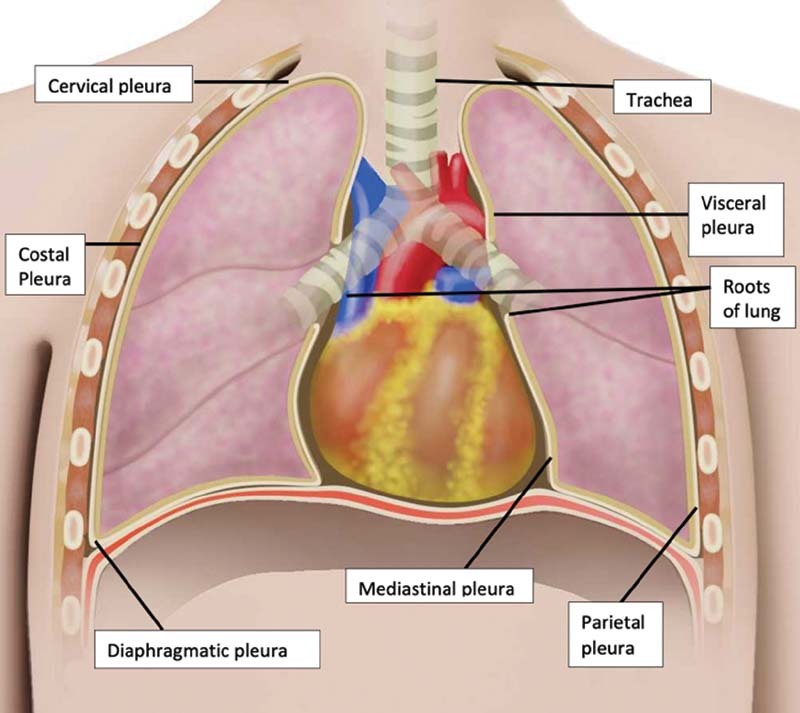
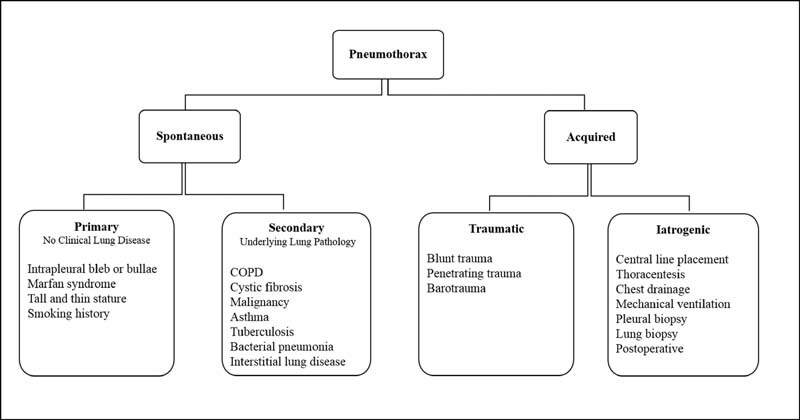
Chest tubes are placed in the pleural space to evacuate abnormal fluid or air accumulations. Various types and sizes of chest tubes are available. Imaging including ultrasound, computed tomography, and fluoroscopy should be used to guide chest tube placement. Understanding the anatomy of the pleural space, along with the etiology and classification of pleural space disease, can help optimize chest tube management. This article will review the indications, contraindications, techniques, and postprocedure follow-up of chest tube placement as well as discuss the management and prevention of complications.
Keywords: interventional radiology; percutaneous chest tube; pleural drain; pleural effusion; pneumothorax; thoracostomy tube.
Thieme. All rights reserved.
Conflict of interest statement
Conflict of Interest None declared.
Figures
Similar articles
-
Limitation of tube thoracostomy in treating pneumothorax in COVID-19 infected patients. A retrospective cohort study.Ann Med Surg (Lond). 2022 Aug;80:104171. doi: 10.1016/j.amsu.2022.104171. Epub 2022 Jul 18. Ann Med Surg (Lond). 2022. PMID: 35875057 Free PMC article.
-
Care of a Chest Tube.2025 Mar 19. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Mar 19. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 32310548 Free Books & Documents.
-
Pneumothorax after small-bore catheter placement for malignant pleural effusions.AJR Am J Roentgenol. 1996 May;166(5):1049-51. doi: 10.2214/ajr.166.5.8615239. AJR Am J Roentgenol. 1996. PMID: 8615239
-
Chest Tubes and Pleural Drainage: History and Current Status in Pleural Disease Management.J Clin Med. 2024 Oct 23;13(21):6331. doi: 10.3390/jcm13216331. J Clin Med. 2024. PMID: 39518470 Free PMC article. Review.
-
Large-bore and small-bore chest tubes: types, function, and placement.Thorac Surg Clin. 2013 Feb;23(1):17-24, v. doi: 10.1016/j.thorsurg.2012.10.006. Thorac Surg Clin. 2013. PMID: 23206714 Review.
References
-
- Albertine K H, Wiener-Kronish J P, Bastacky J, Staub N C. No evidence for mesothelial cell contact across the costal pleural space of sheep. J Appl Physiol (1985) 1991;70(01):123–134. - PubMed
-
- Light R W, Macgregor M I, Luchsinger P C, Ball W C., Jr Pleural effusions: the diagnostic separation of transudates and exudates. Ann Intern Med. 1972;77(04):507–513. - PubMed
-
- Vives M, Porcel J M, Vicente de Vera M, Ribelles E, Rubio M. A study of Light's criteria and possible modifications for distinguishing exudative from transudative pleural effusions. Chest. 1996;109(06):1503–1507. - PubMed
-
- Blackmore C C, Black W C, Dallas R V, Crow H C. Pleural fluid volume estimation: a chest radiograph prediction rule. Acad Radiol. 1996;3(02):103–109. - PubMed
