

Review
doi: 10.1055/s-0042-1751293.
eCollection 2022 Jun.
Bronchial Artery Embolization
Affiliations
- PMID: 36062235
- PMCID: PMC9433160
- DOI: 10.1055/s-0042-1751293
Item in Clipboard
Review
Bronchial Artery Embolization
Semin Intervent Radiol.
.
Abstract
Massive hemoptysis is a highly morbid medical condition with up to 75% mortality with conservative treatment. Bronchial artery embolization has emerged as the common treatment for both acute massive hemoptysis and chronic hemoptysis. This article will review the clinical presentation, bronchial artery anatomy, embolization procedure, complications, and expected outcomes.
Keywords: bronchial artery embolization; embolization; hemoptysis; interventional radiology.
Thieme. All rights reserved.
Conflict of interest statement
Conflict of Interest None declared.
Figures
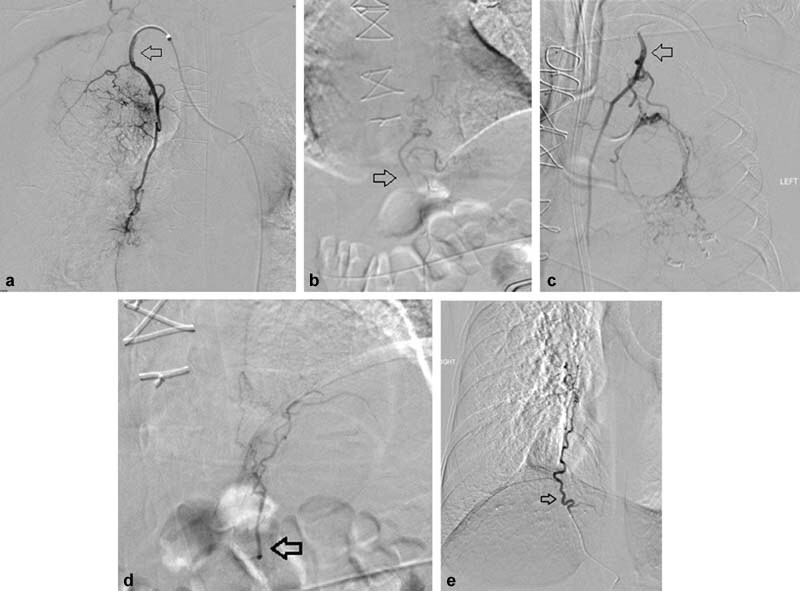
Ectopic bronchial arteries. (
a
) A 59-year-old man with massive hemoptysis in the setting of recent pulmonary thromboendarterectomy for chronic thromboembolic pulmonary hypertension was found to have multiple ectopic bronchial arteries (shown originating from the right internal mammary artery—arrow). (
b
) An ectopic left bronchial artery originating from the left gastric artery in the same patient. (
c
) The ectopic left bronchial originating from the left internal mammary artery in the same patient. (
d
) An ectopic left bronchial artery from the left phrenic in the same patient (arrow). (
e
) A 26-year-old woman with cystic fibrosis found to have an ectopic right bronchial artery from the right phrenic artery (arrow).

A 59-year-old man with massive hemoptysis from the right lung. (
a
) The patient was found to have an ectopic right bronchial artery originating from the brachiocephalic artery (arrow). (
b
) Right radial access was subsequently utilized to successfully select and embolize the ectopic bronchial artery (arrow).
(
a
) Flush thoracic aortogram demonstrates bilateral hypertrophied bronchial arteries in a 25-year-old man with cystic fibrosis and massive hemoptysis. Note the right bronchial artery has an ectopic origin from the underside of the aortic arch (arrow). (
b
) Selective angiogram of the abnormal, hypertrophied left bronchial artery. (
c
) Selective angiogram of the ectopic right bronchial artery shows a dilated, ectatic vessel with hyperemia.

Flush aortogram prior to bronchial artery embolization shows bilateral intercostal arteries and an abnormal right bronchial artery with conventional anatomy (arrow).

A 61-year-old man presented with massive hemoptysis with angiogram of the left superior bronchial artery showing opacification of the anterior spinal artery with the characteristic hairpin turn (arrow). No embolization was performed of this vessel.
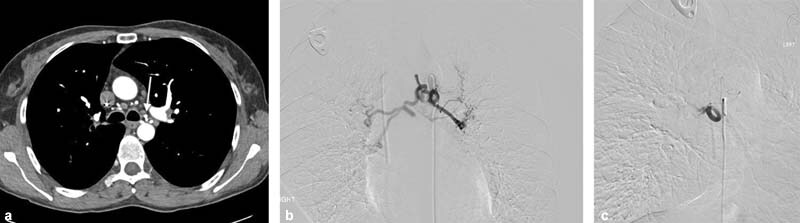
A 41-year-old woman with history of cystic fibrosis presenting with massive hemoptysis. (
a
) CT angiogram reveals enlarged, ectatic bronchial arteries with one origin from the ventral thoracic aorta at the level of the carina (arrow). (
b
) Selective angiogram demonstrates enlarged right and left bronchial arteries with a common origin from the aorta. (
c
) Selective angiogram of the right bronchial artery post-embolization shows pruning of the vasculature.

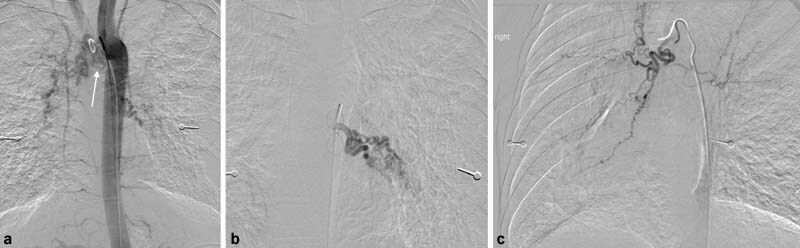
An 87-year-old man with a history of pulmonary embolism presenting with hemoptysis with angiogram showing significant left bronchial artery (black arrow) to pulmonary artery shunting (white arrow).

A 57-year-old man status post-BAE for massive hemoptysis with paralysis. MRI demonstrates the classic high T2 signal “owl-eye appearance” on axial T2-weighted imaging (circle) seen with infarction of the anterior spinal artery. (Image courtesy of Keith Quencer, MD.)
References
-
- Davidson K, Shojaee S. Managing massive hemoptysis. Chest. 2020;157(01):77–88. - PubMed
-
- Ong T H, Eng P. Massive hemoptysis requiring intensive care. Intensive Care Med. 2003;29(02):317–320. - PubMed
-
- Reechaipichitkul W, Latong S. Etiology and treatment outcomes of massive hemoptysis. Southeast Asian J Trop Med Public Health. 2005;36(02):474–480. - PubMed
-
- Najarian K E, Morris C S. Arterial embolization in the chest. J Thorac Imaging. 1998;13(02):93–104. - PubMed