

Vasopressin Response and Clinical Trajectory in Septic Shock Patients
- PMID: 36062611
- PMCID: PMC10236982
- DOI: 10.1177/08850666221118282
Vasopressin Response and Clinical Trajectory in Septic Shock Patients
Abstract
Background: In septic shock, vasopressors aim to improve tissue perfusion and prevent persistent organ dysfunction, a characteristic of chronic critical illness (CCI). Adjunctive vasopressin is often used to decrease catecholamine dosage, but the association of vasopressin response with subsequent patient outcomes is unclear. We hypothesized vasopressin response is associated with favorable clinical trajectory.
Methods: We included patients with septic shock receiving vasopressin as a catecholamine adjunct in this retrospective cohort study. We defined vasopressin response as a lowering of the catecholamine dose required to maintain mean arterial pressure ≥65 mm Hg, 6 h after vasopressin initiation. Clinical trajectories were adjudicated as early death (ED; death before day 14), CCI (ICU stay ≥14 days with persistent organ dysfunction), or rapid recovery (RR; not meeting ED or CCI criteria). Trajectories were placed on an ordinal scale with ED the worst outcome, CCI next, and RR the best outcome. The association of vasopressin response with clinical trajectory was assessed with multivariable ordinal logistic regression.
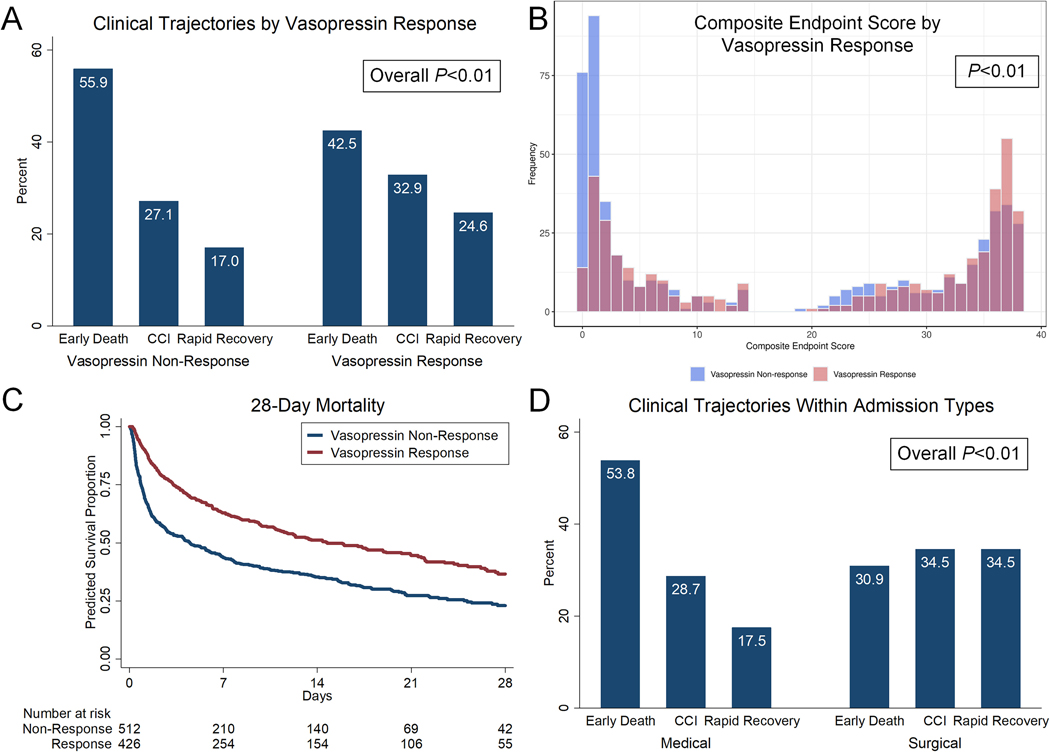
Results: In total 938 patients were included; 426 (45.4%) were vasopressin responders. The most frequent trajectory was ED (49.8%), 29.7% developed CCI, and 20.5% had rapid recovery. In survivors to ICU day 14 (those without ED), 59.2% had CCI and 40.8% experienced RR. Compared with vasopressin non-responders, vasopressin responders less frequently experienced ED (42.5% vs. 55.9%) and more frequently experienced RR (24.6% vs. 17.0%; P < 0.01). After controlling for confounders, vasopressin response was independently associated with higher odds of developing a better clinical trajectory (OR 1.63; 95% CI 1.26-2.10). Medical patients most frequently developed ED and survivors more commonly developed CCI than RR; surgical patients developed the three trajectories with similar frequency (P < 0.01).
Conclusions: Vasopressin responsive status was associated with improved clinical trajectory in septic shock patients. Early vasopressin response is a potential novel prognostic marker for short-term clinical trajectory.
Keywords: chronic critical illness; clinical trajectory; sepsis; septic shock; vasoconstrictor agents; vasopressin.
Conflict of interest statement
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Liu V, Escobar GJ, Greene JD, et al. Hospital deaths in patients withsepsis from 2 independent cohorts. JAMA. 2014;312(1):90–92. - PubMed
-
- Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Crit Care Med. 2021;49(11):e1063–e1143. - PubMed
-
- Sacha GL, Kiser TH, Wright GC, et al. Association between vasopressin rebranding and utilization in patients with septic shock. Crit Care Med. 2022;50(4):644–654. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
