

Elements of morphology: Standard terminology for the trunk and limbs
- PMID: 36062894
- PMCID: PMC9582996
- DOI: 10.1002/ajmg.a.62965
Elements of morphology: Standard terminology for the trunk and limbs
Abstract
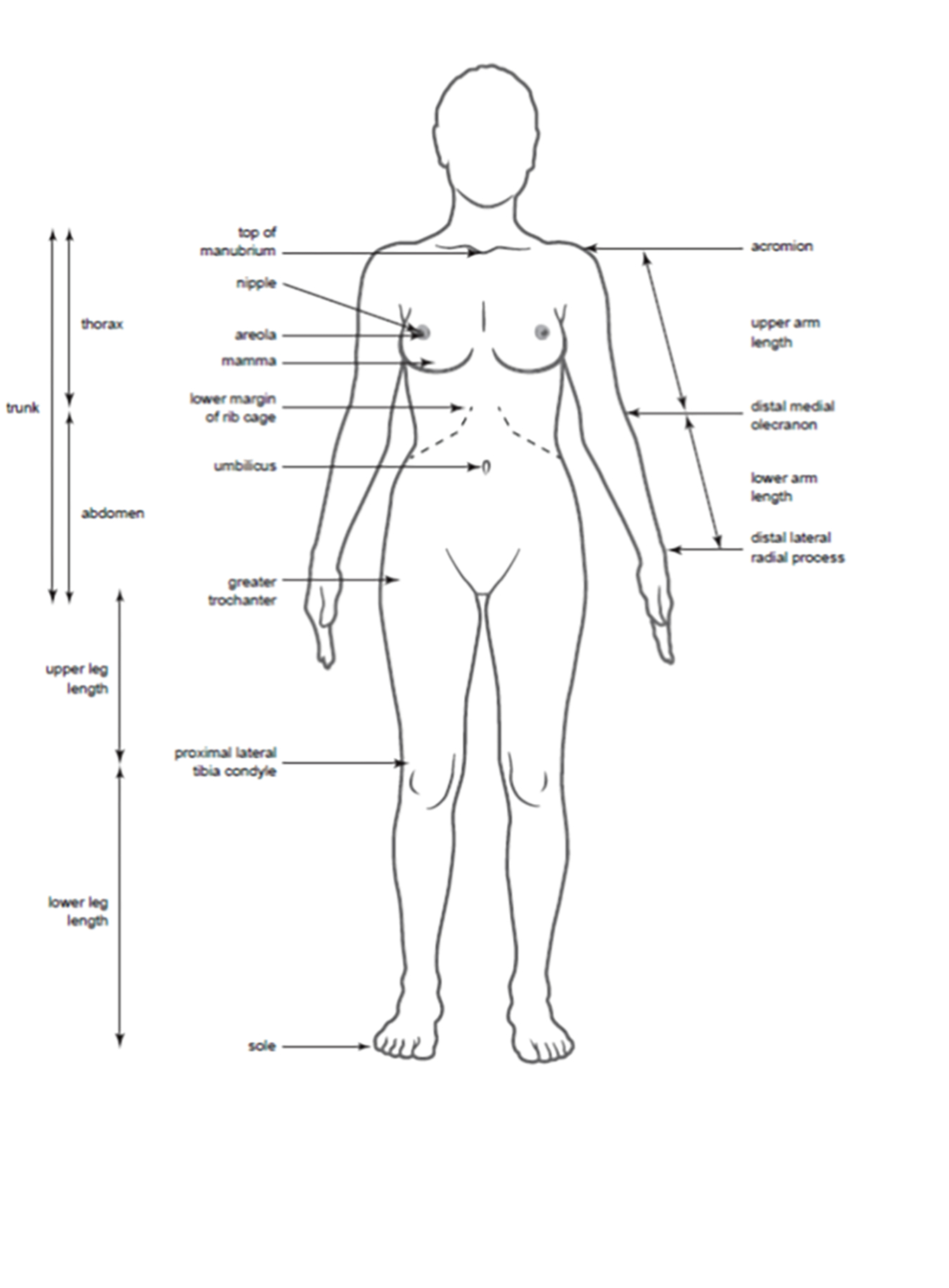
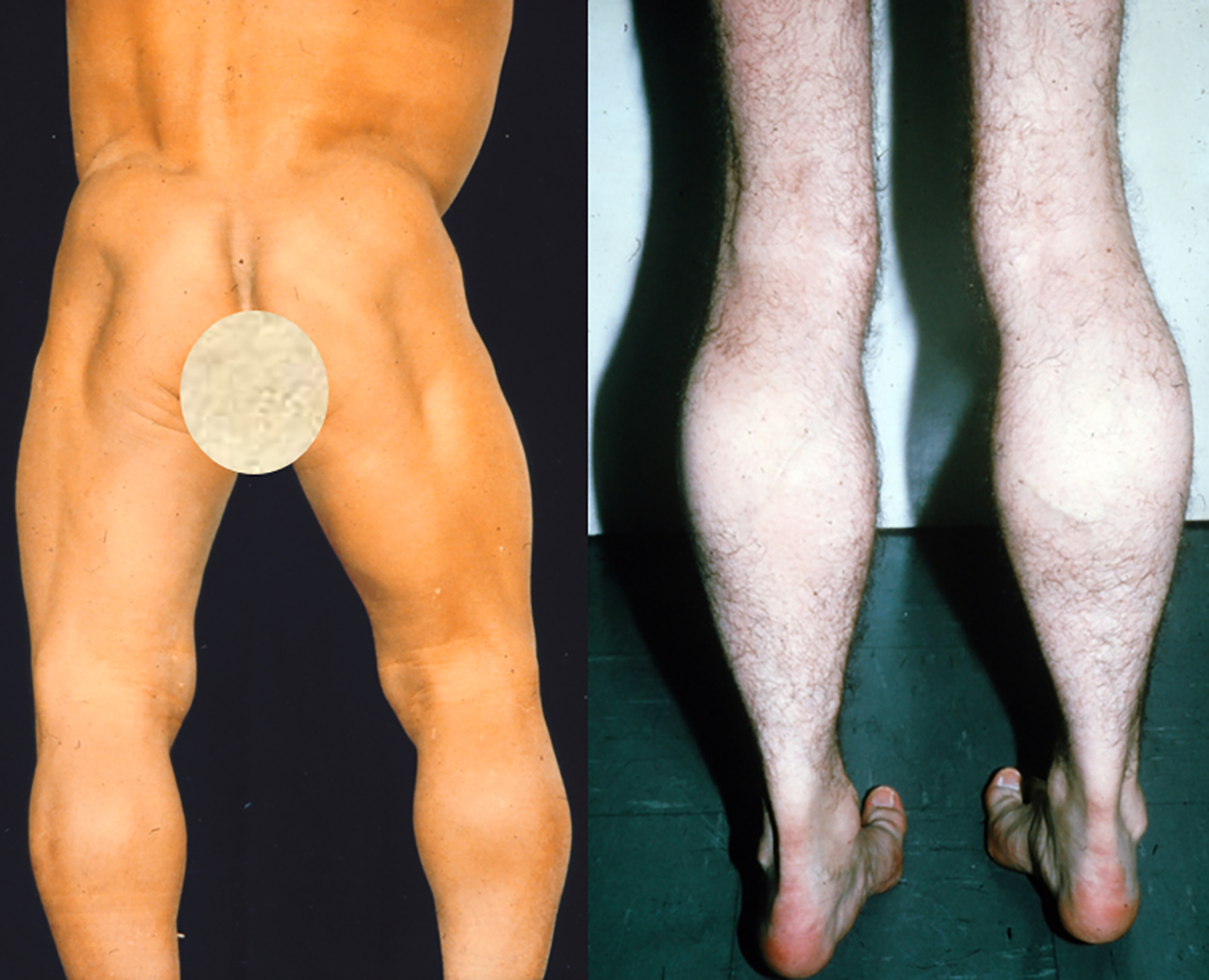
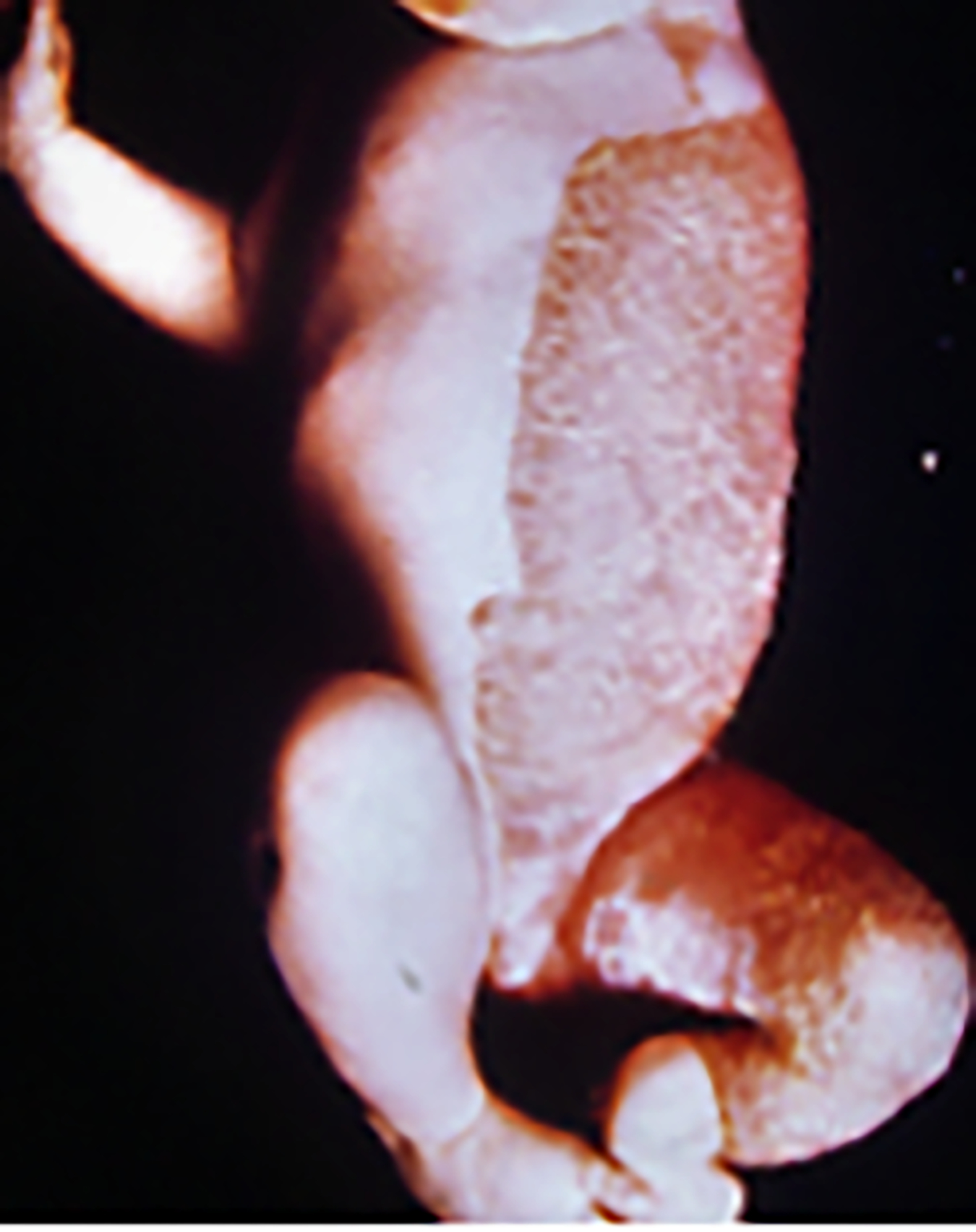
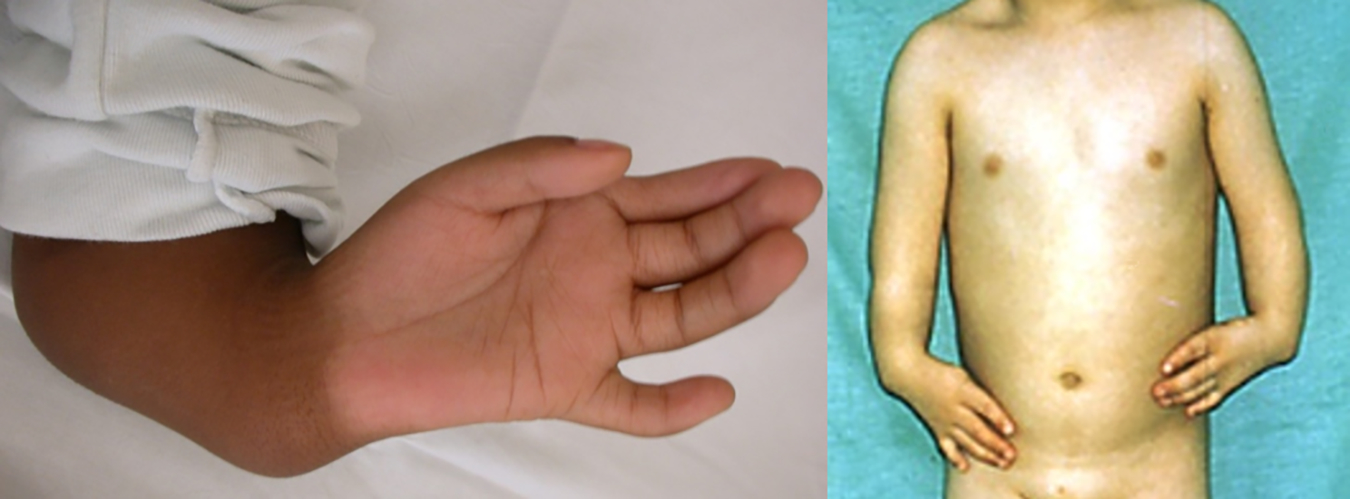
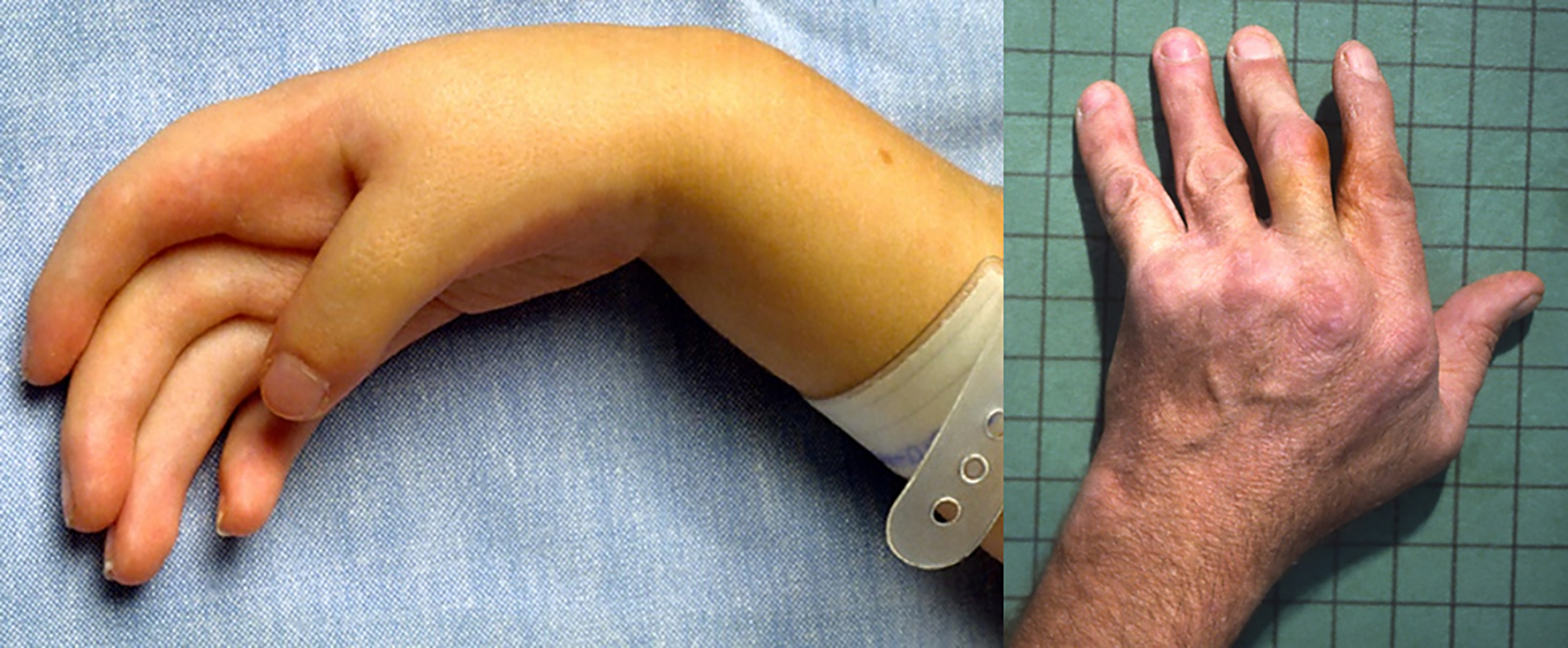
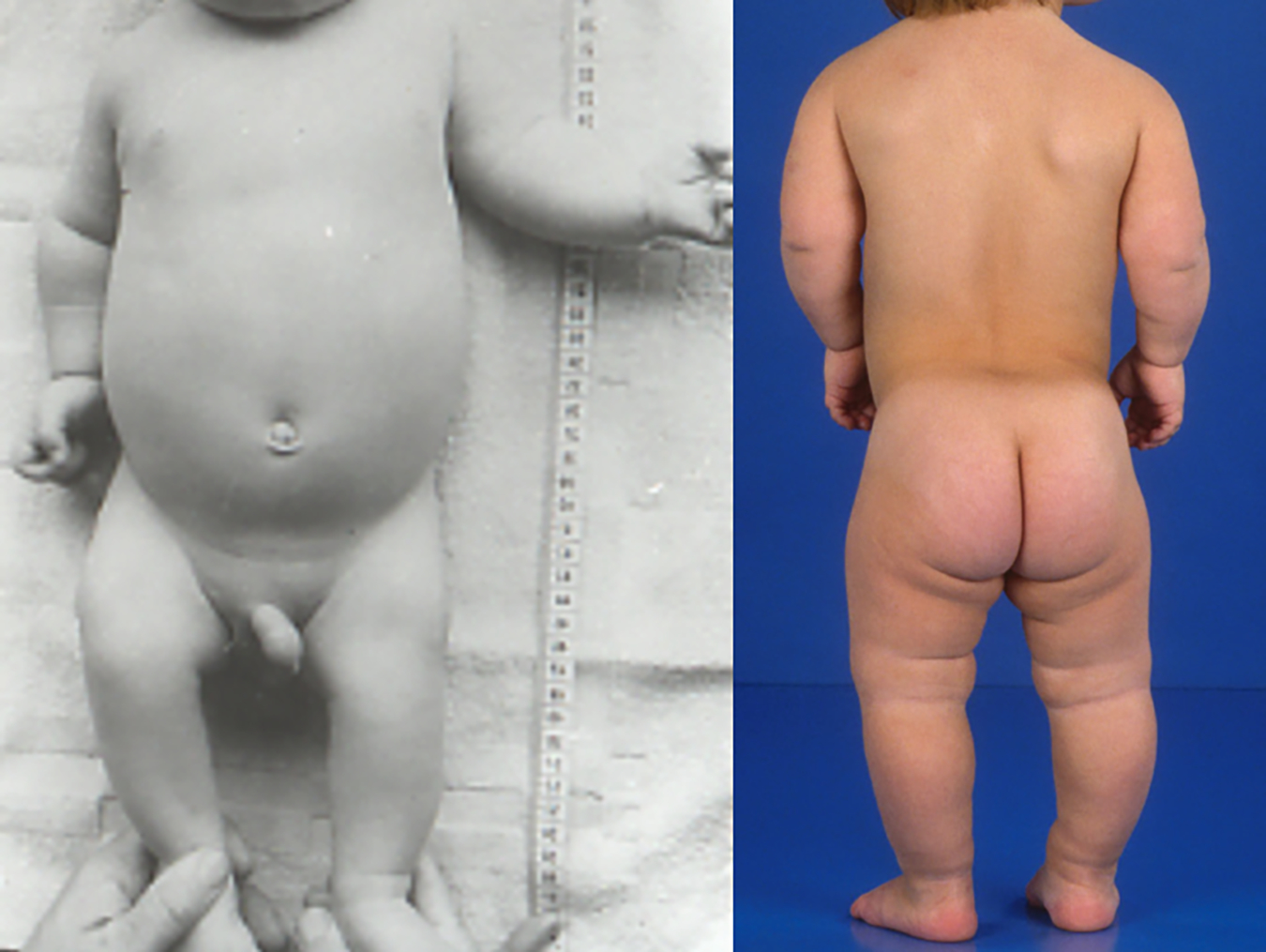
An international group of clinicians working in the field of dysmorphology has initiated the standardization of terms used to describe human morphology. The goals are to standardize these terms and reach consensus regarding their definitions. In this way, we will increase the utility of descriptions of the human phenotype and facilitate reliable comparisons of findings among patients. Additional discussions with other workers in dysmorphology and related fields, such as developmental biology and molecular genetics, will become more precise. Here we introduce the anatomy of the trunk and limbs and define and illustrate the terms that describe the major characteristics of these body regions.
Keywords: anatomy; anthropometry; classification; dysmorphology; elements of morphology; nomenclature.
© 2022 Wiley Periodicals LLC.
Conflict of interest statement
Figures






















































































Similar articles
-
Elements of morphology: standard terminology for the ear.Am J Med Genet A. 2009 Jan;149A(1):40-60. doi: 10.1002/ajmg.a.32599. Am J Med Genet A. 2009. PMID: 19152421
-
Elements of morphology: standard terminology for the external genitalia.Am J Med Genet A. 2013 Jun;161A(6):1238-63. doi: 10.1002/ajmg.a.35934. Epub 2013 May 6. Am J Med Genet A. 2013. PMID: 23650202 Free PMC article.
-
Elements of morphology: standard terminology for the lips, mouth, and oral region.Am J Med Genet A. 2009 Jan;149A(1):77-92. doi: 10.1002/ajmg.a.32602. Am J Med Genet A. 2009. PMID: 19125428
-
Nomenclature of Cutaneous Vasculitis: Dermatologic Addendum to the 2012 Revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides.Arthritis Rheumatol. 2018 Feb;70(2):171-184. doi: 10.1002/art.40375. Arthritis Rheumatol. 2018. PMID: 29136340 Review.
-
An International Terminology for Endometriosis, 2021.J Minim Invasive Gynecol. 2021 Nov;28(11):1849-1859. doi: 10.1016/j.jmig.2021.08.032. Epub 2021 Oct 21. J Minim Invasive Gynecol. 2021. PMID: 34690084 Review.
Cited by
-
Abnormal dental phenotypes in GAPO syndrome: A descriptive study with a new ANTXR1 variant & insights on teeth eruption.Saudi Dent J. 2024 Sep;36(9):1209-1214. doi: 10.1016/j.sdentj.2024.07.001. Epub 2024 Jul 2. Saudi Dent J. 2024. PMID: 39286584 Free PMC article.
-
Human Phenotype Ontology Annotations for Rare Congenital Conditions: Application to Arthrogryposis Multiplex Congenita.Am J Med Genet A. 2025 Aug;197(8):e64067. doi: 10.1002/ajmg.a.64067. Epub 2025 Apr 3. Am J Med Genet A. 2025. PMID: 40176701 Free PMC article.
-
Enhancing Molecular Testing for Effective Delivery of Actionable Gene Diagnostics.Bioengineering (Basel). 2022 Dec 1;9(12):745. doi: 10.3390/bioengineering9120745. Bioengineering (Basel). 2022. PMID: 36550951 Free PMC article. Review.
References
-
- Ambardar S, Cabot J, Cekic V, Baxter K, Arnell TD, Forde KA, Nihalani A, Whelan RL. (2009). Abdominal wall dimensions and umbilical position vary widely with BMI and should be taken into account when choosing port locations. Surg Endosc 23(9):1995–2000. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
