

Right dose, right now: bedside, real-time, data-driven, and personalised antibiotic dosing in critically ill patients with sepsis or septic shock-a two-centre randomised clinical trial
- PMID: 36064438
- PMCID: PMC9443636
- DOI: 10.1186/s13054-022-04098-7
Right dose, right now: bedside, real-time, data-driven, and personalised antibiotic dosing in critically ill patients with sepsis or septic shock-a two-centre randomised clinical trial
Abstract
Background: Adequate antibiotic dosing may improve outcomes in critically ill patients but is challenging due to altered and variable pharmacokinetics. To address this challenge, AutoKinetics was developed, a decision support system for bedside, real-time, data-driven and personalised antibiotic dosing. This study evaluates the feasibility, safety and efficacy of its clinical implementation.
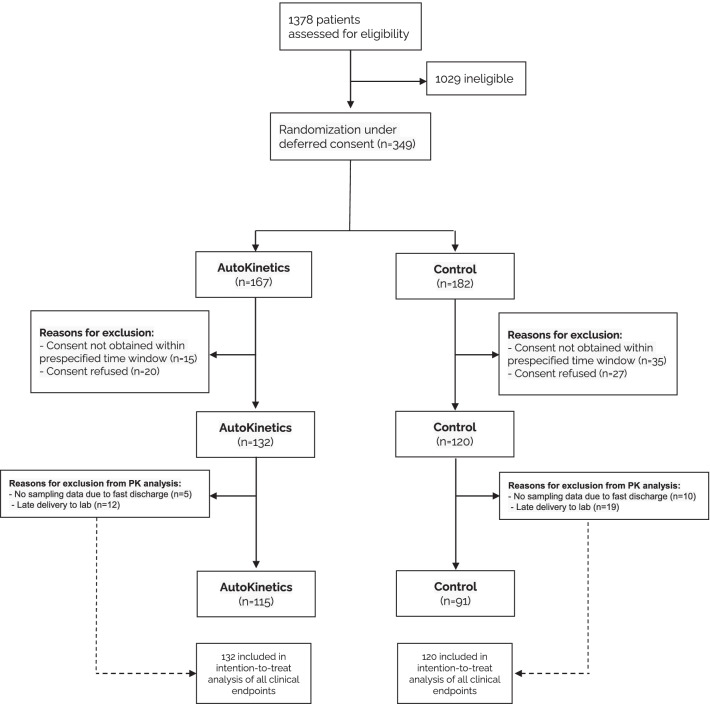
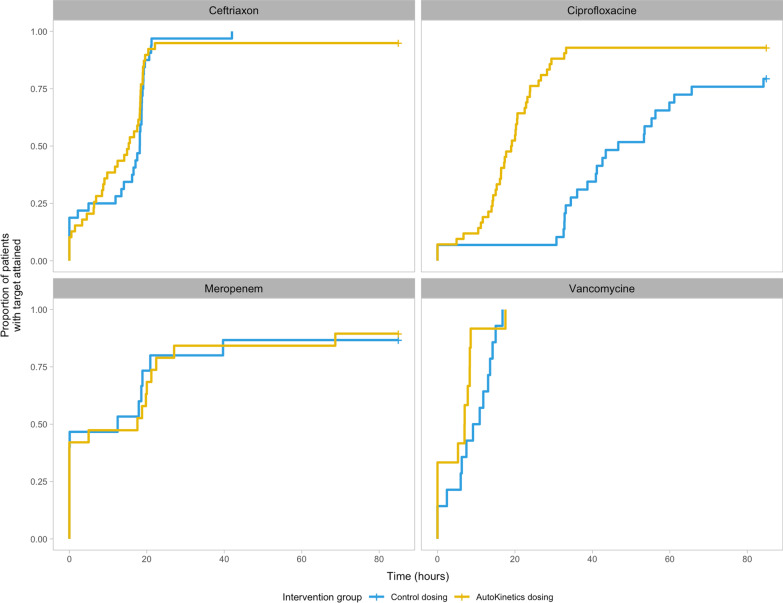
Methods: In this two-centre randomised clinical trial, critically ill patients with sepsis or septic shock were randomised to AutoKinetics dosing or standard dosing for four antibiotics: vancomycin, ciprofloxacin, meropenem, and ceftriaxone. Adult patients with a confirmed or suspected infection and either lactate > 2 mmol/L or vasopressor requirement were eligible for inclusion. The primary outcome was pharmacokinetic target attainment in the first 24 h after randomisation. Clinical endpoints included mortality, ICU length of stay and incidence of acute kidney injury.
Results: After inclusion of 252 patients, the study was stopped early due to the COVID-19 pandemic. In the ciprofloxacin intervention group, the primary outcome was obtained in 69% compared to 3% in the control group (OR 62.5, CI 11.4-1173.78, p < 0.001). Furthermore, target attainment was faster (26 h, CI 18-42 h, p < 0.001) and better (65% increase, CI 49-84%, p < 0.001). For the other antibiotics, AutoKinetics dosing did not improve target attainment. Clinical endpoints were not significantly different. Importantly, higher dosing did not lead to increased mortality or renal failure.
Conclusions: In critically ill patients, personalised dosing was feasible, safe and significantly improved target attainment for ciprofloxacin.
Trial registration: The trial was prospectively registered at Netherlands Trial Register (NTR), NL6501/NTR6689 on 25 August 2017 and at the European Clinical Trials Database (EudraCT), 2017-002478-37 on 6 November 2017.
Keywords: Clinical decision support; Pharmacokinetics; Sepsis; Therapeutic drug monitoring.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
