

Translational development of ABCB5+ dermal mesenchymal stem cells for therapeutic induction of angiogenesis in non-healing diabetic foot ulcers
- PMID: 36064604
- PMCID: PMC9444095
- DOI: 10.1186/s13287-022-03156-9
Translational development of ABCB5+ dermal mesenchymal stem cells for therapeutic induction of angiogenesis in non-healing diabetic foot ulcers
Abstract
Background: While rapid healing of diabetic foot ulcers (DFUs) is highly desirable to avoid infections, amputations and life-threatening complications, DFUs often respond poorly to standard treatment. GMP-manufactured skin-derived ABCB5+ mesenchymal stem cells (MSCs) might provide a new adjunctive DFU treatment, based on their remarkable skin wound homing and engraftment potential, their ability to adaptively respond to inflammatory signals, and their wound healing-promoting efficacy in mouse wound models and human chronic venous ulcers.
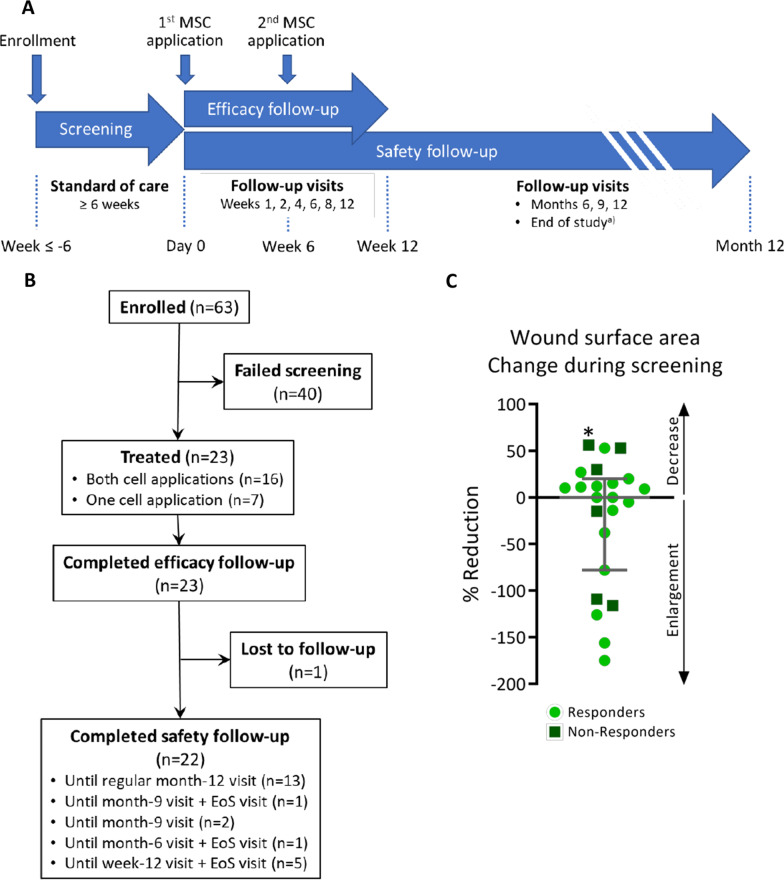
Methods: The angiogenic potential of ABCB5+ MSCs was characterized with respect to angiogenic factor expression at the mRNA and protein level, in vitro endothelial trans-differentiation and tube formation potential, and perfusion-restoring capacity in a mouse hindlimb ischemia model. Finally, the efficacy and safety of ABCB5+ MSCs for topical adjunctive treatment of chronic, standard therapy-refractory, neuropathic plantar DFUs were assessed in an open-label single-arm clinical trial.
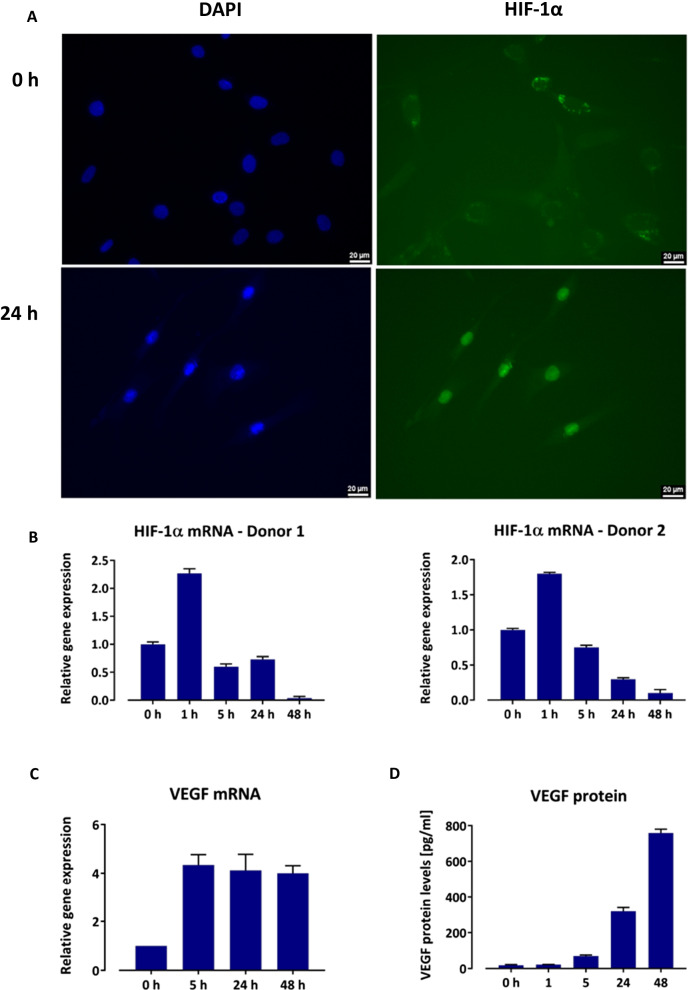
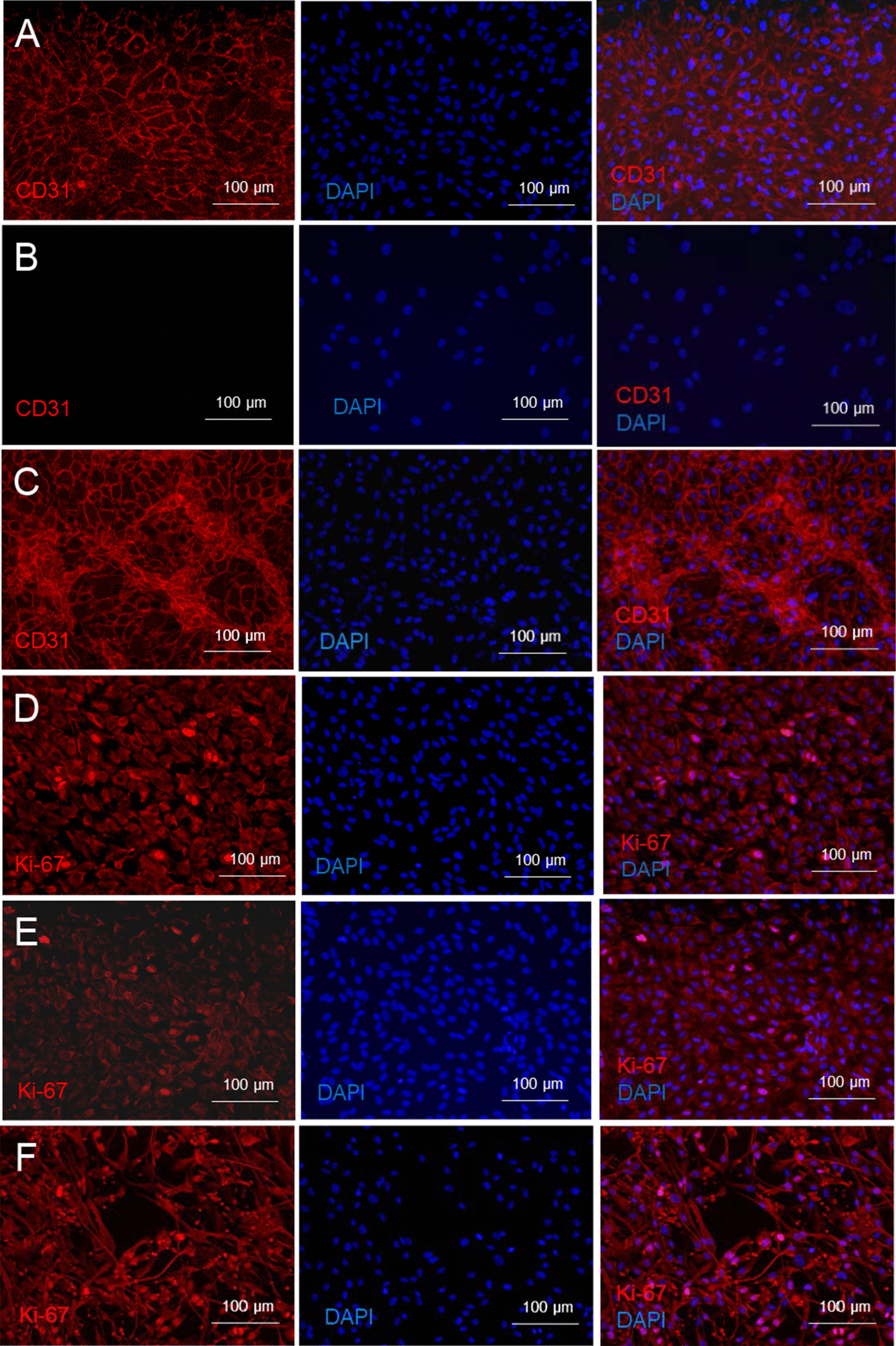
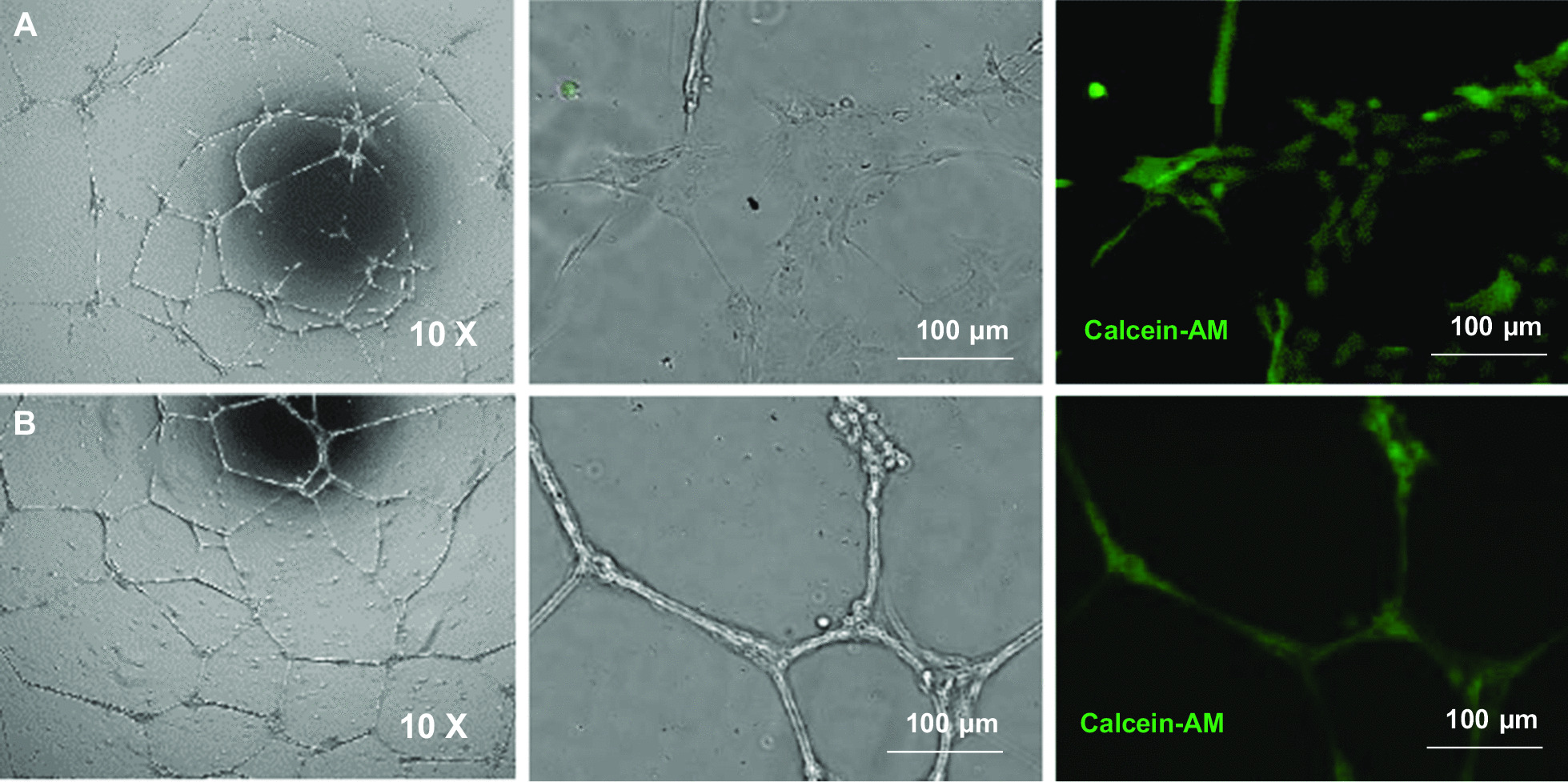
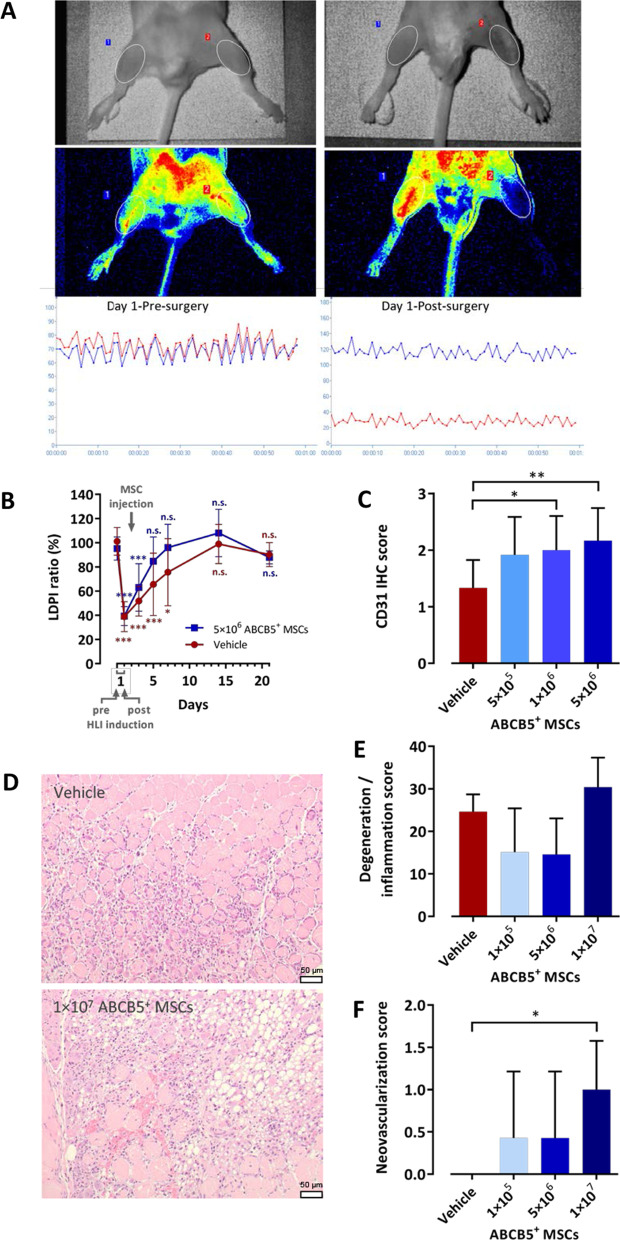
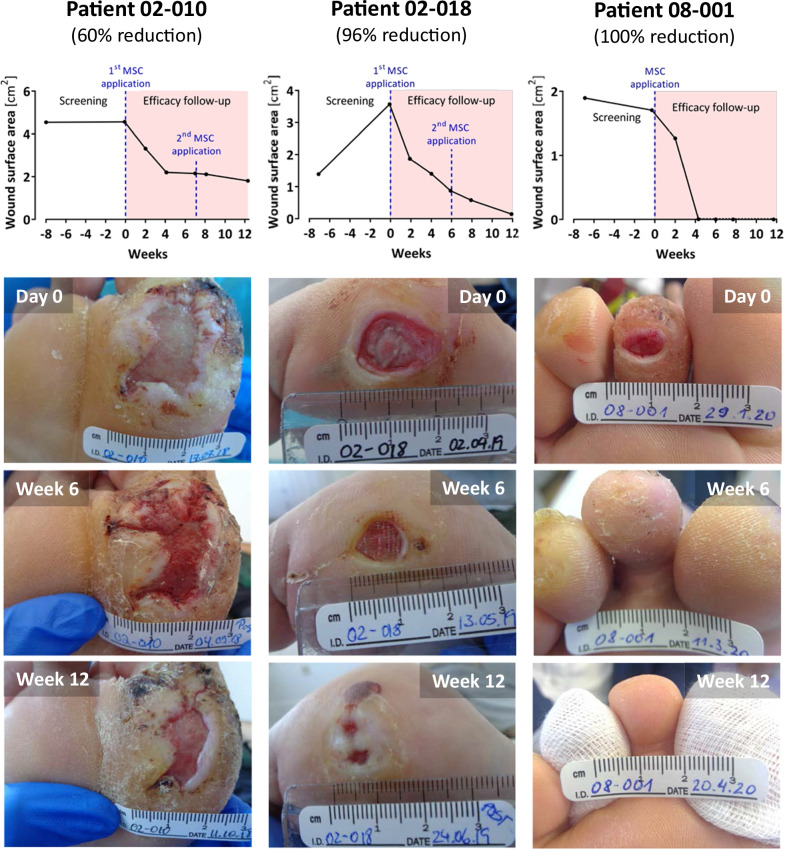
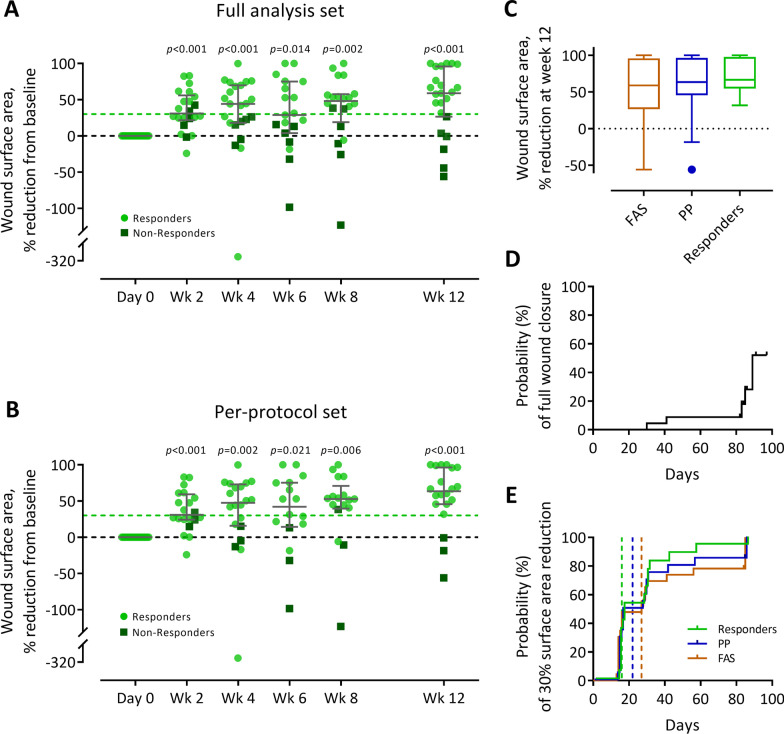
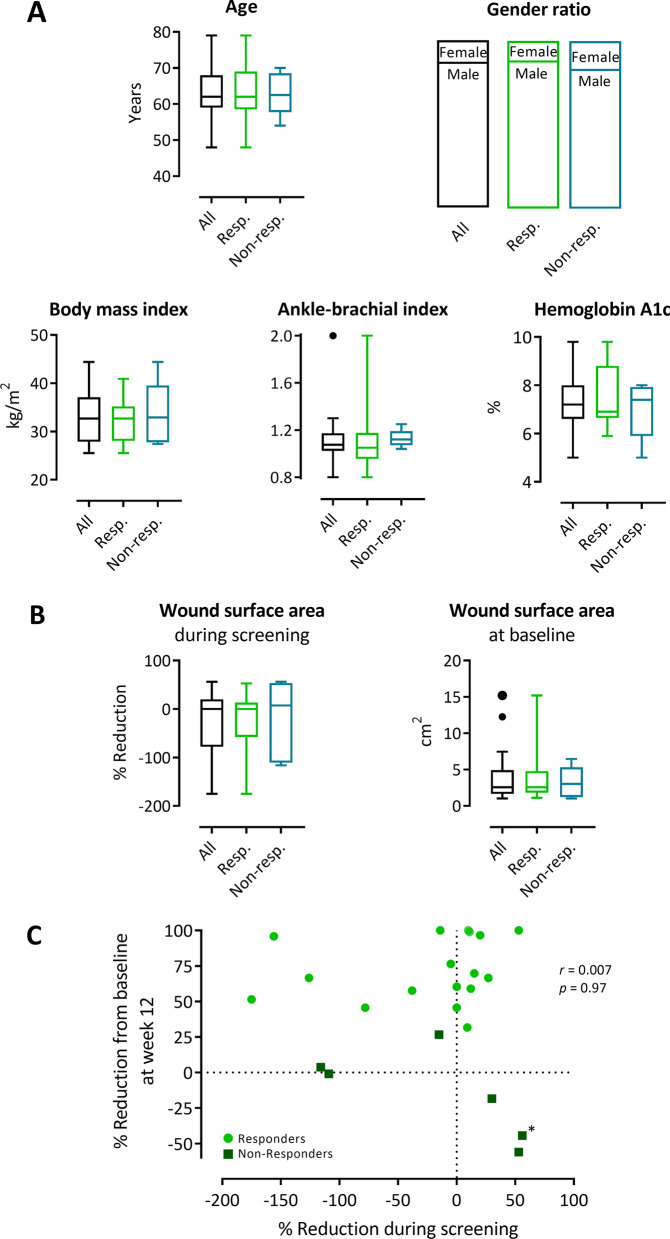
Results: Hypoxic incubation of ABCB5+ MSCs led to posttranslational stabilization of the hypoxia-inducible transcription factor 1α (HIF-1α) and upregulation of HIF-1α mRNA levels. HIF-1α pathway activation was accompanied by upregulation of vascular endothelial growth factor (VEGF) transcription and increase in VEGF protein secretion. Upon culture in growth factor-supplemented medium, ABCB5+ MSCs expressed the endothelial-lineage marker CD31, and after seeding on gel matrix, ABCB5+ MSCs demonstrated formation of capillary-like structures comparable with human umbilical vein endothelial cells. Intramuscularly injected ABCB5+ MSCs to mice with surgically induced hindlimb ischemia accelerated perfusion recovery as measured by laser Doppler blood perfusion imaging and enhanced capillary proliferation and vascularization in the ischemic muscles. Adjunctive topical application of ABCB5+ MSCs onto therapy-refractory DFUs elicited median wound surface area reductions from baseline of 59% (full analysis set, n = 23), 64% (per-protocol set, n = 20) and 67% (subgroup of responders, n = 17) at week 12, while no treatment-related adverse events were observed.
Conclusions: The present observations identify GMP-manufactured ABCB5+ dermal MSCs as a potential, safe candidate for adjunctive therapy of otherwise incurable DFUs and justify the conduct of a larger, randomized controlled trial to validate the clinical efficacy.
Trial registration: ClinicalTrials.gov, NCT03267784, Registered 30 August 2017, https://clinicaltrials.gov/ct2/show/NCT03267784.
Keywords: ABCB5; Advanced-therapy medicinal product; Angiogenesis; Chronic wound; Diabetic foot ulcer; Mesenchymal stem cells; Wound healing.
© 2022. The Author(s).
Conflict of interest statement
MHF and NYF are inventors or co-inventors of US and international patents assigned to Brigham and Women’s Hospital and/or Boston Children’s Hospital (Boston, MA, USA), licensed to TICEBA GmbH (Heidelberg, Germany) and RHEACELL GmbH & Co. KG (Heidelberg, Germany). MHF and KSK serve as scientific advisors to TICEBA and RHEACELL and participate in corporate-sponsored research collaborations with RHEACELL. ENR, SK, JE, SS and SB are employees of TICEBA. KD, KK and HMS are employees of RHEACELL. CG is CEO, and MAK is CSO of TICEBA and RHEACELL. The remaining authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
