

Clinical and microbiological characteristics of and risk factors for bloodstream infections among patients with extracorporeal membrane oxygenation: a single-center retrospective cohort study
- PMID: 36064957
- PMCID: PMC9445101
- DOI: 10.1038/s41598-022-19405-z
Clinical and microbiological characteristics of and risk factors for bloodstream infections among patients with extracorporeal membrane oxygenation: a single-center retrospective cohort study
Abstract
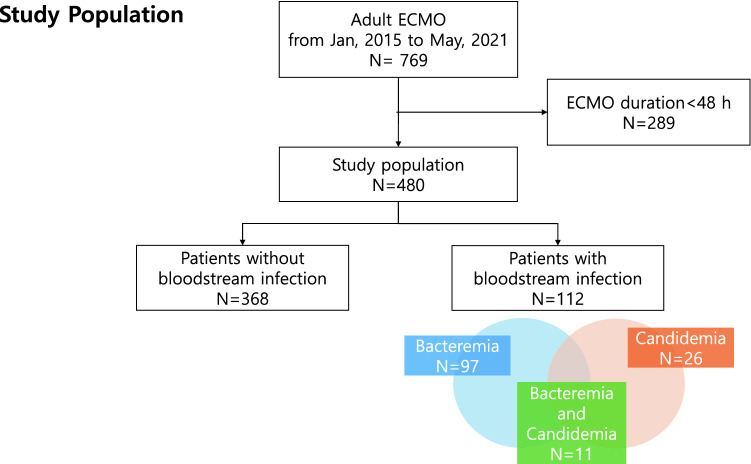
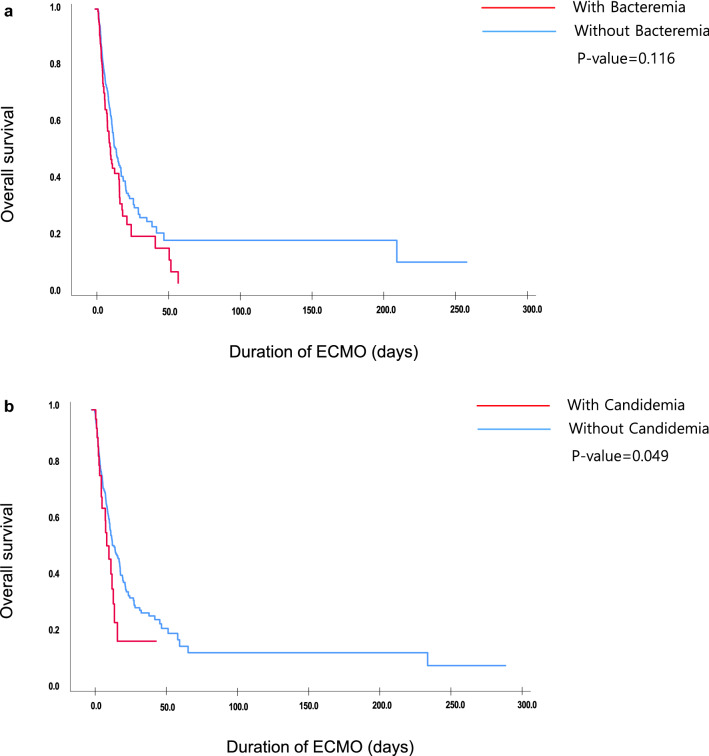
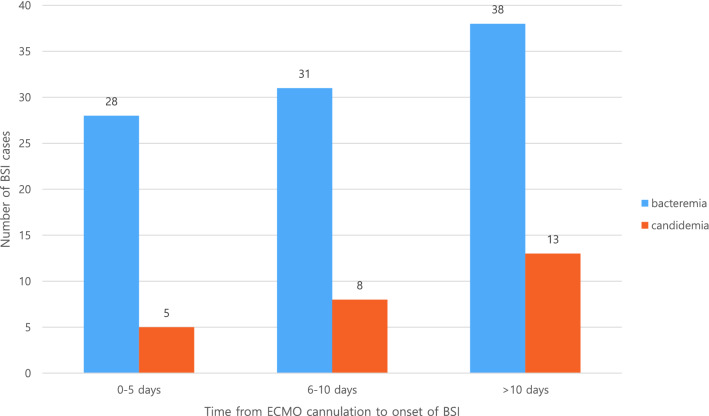
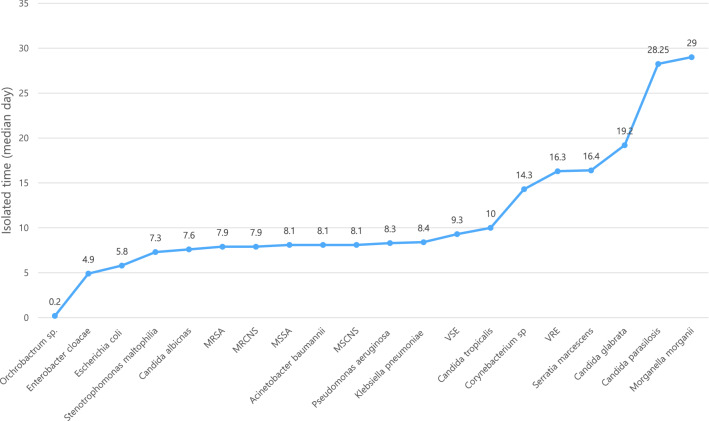
Extracorporeal membrane oxygenation (ECMO) provides hemodynamic and oxygenation support to critically ill patients. Due to multiple catheter cannulations, patients on ECMO are vulnerable to bloodstream infections (BSIs). We aimed to investigate the incidence, clinical characteristics, risk factors, and microorganisms associated with BSIs during ECMO. This single-center retrospective cohort study was conducted between January 2015 and May 2021. Patients aged 18 years or older with an ECMO duration of > 48 h for cardiogenic or respiratory support were included in the study. Patients who developed bacteremia or candidemia from 12 h after ECMO cannulation to 7 days after de-cannulation were included. The clinical factors between non-BSI and BSI were compared, along with an analysis of the risk factors associated with BSI during ECMO. A total of 480 patients underwent ECMO for cardiogenic shock (n = 267, 55.6%) or respiratory failure (n = 213, 44.4%) during the study period. The incidence was 20.0 episodes per 1000 ECMO-days. Approximately 20.2% (97/480) and 5.4% (26/480) of the patients developed bacteremia and candidemia, respectively. The median numbers of days of BSI development were 8.00 days for bacteremia and 11.0 days for candidemia. The most common pathogens were methicillin-resistant coagulase-negative staphylococci (n = 24), followed by vancomycin-resistant Enterococcus (n = 21). Multivariable logistic analysis demonstrated that hemodialysis (odds ratio [OR] 2.647, p < 0.001), veno-arterial-venous mode (OR 1.911, p = 0.030), and total ECMO duration (OR 1.030, p = 0.007) were significant risk factors for bacteremia. The total ECMO duration was the only risk factor associated with candidemia (OR 1.035, p = 0.010). The mortality rate was significantly higher in the bacteremia (57.7%) and candidemia (69.2%) groups than that in the non-BSI group (43.6%). BSI is a common complication of patients receiving ECMO support and is associated with poor clinical outcomes. Determining the type of frequently isolated organisms and the median onset time of BSI would help in the selection of appropriate prophylactic antibiotics or antifungal agents.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
