

High-Flow Nasal Cannula Oxygen Therapy versus Non-Invasive Ventilation for AECOPD Patients After Extubation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
- PMID: 36065316
- PMCID: PMC9440713
- DOI: 10.2147/COPD.S375107
High-Flow Nasal Cannula Oxygen Therapy versus Non-Invasive Ventilation for AECOPD Patients After Extubation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Abstract
Objective: To evaluate the clinical efficacy of high-flow nasal oxygen therapy (HFNC) and non-invasive ventilation (NIV) in patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD) after extubation.
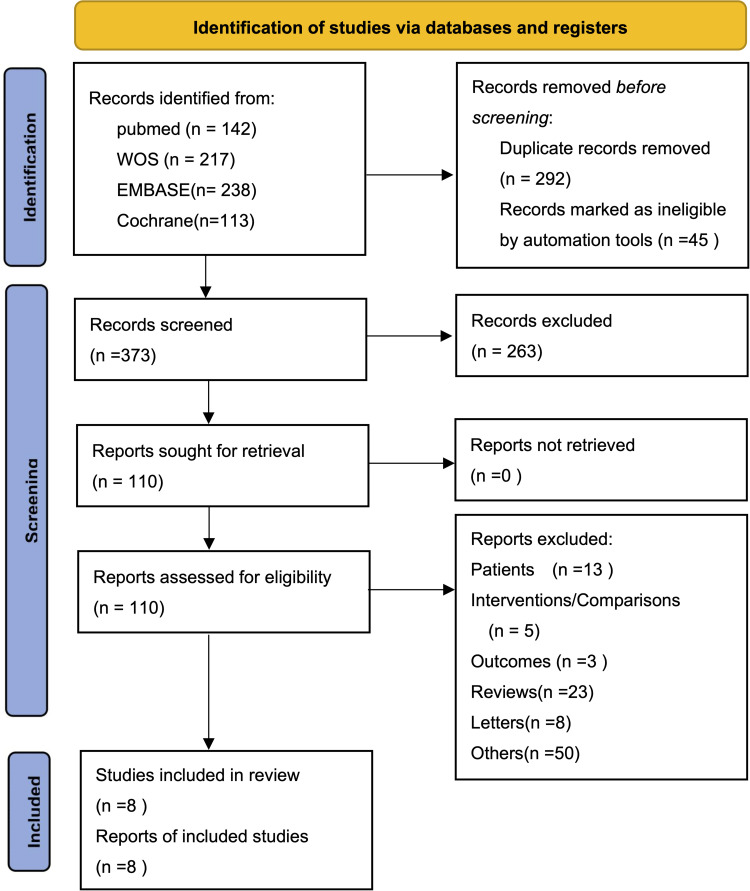
Research methods: This systematic review and meta-analysis was conducted following the Preferred Reporting Items for Systematic Review and Meta-analyses (PRISMA) statements. The primary outcome measures analyzed included: reintubation rate, mortality, complication rate, and ICU length of stay.
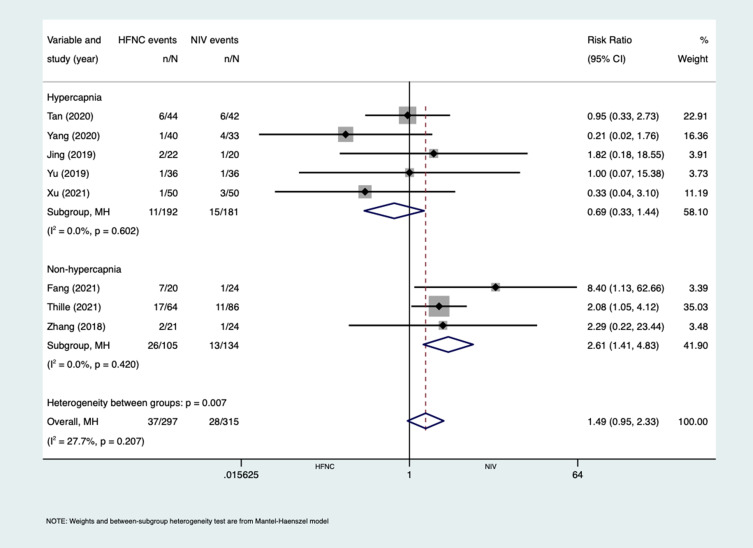
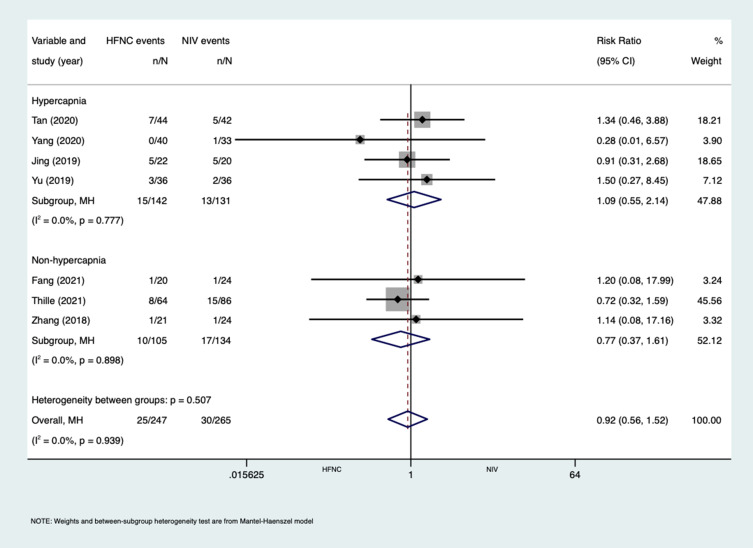
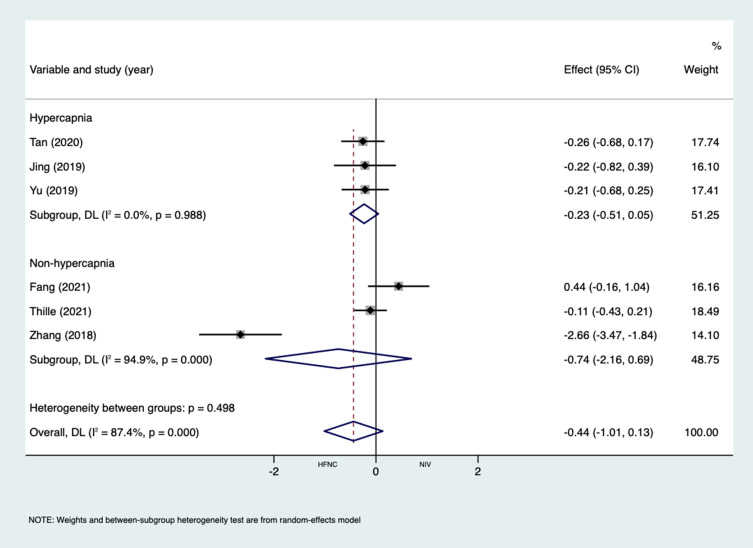
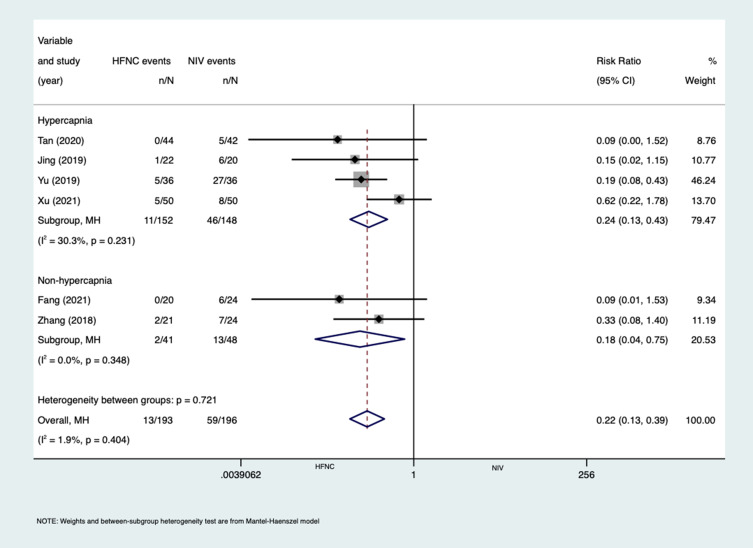
Results: Eight studies were included, with a total of 612 subjects, including 297 in the HFNC group and 315 in the NIV group. The effect of HFNC and NIV on the reintubation rate of AECOPD patients after extubation, RR (1.49 [95% CI,0.95 to 2.33], P = 0.082). Subgroup analysis with or without hypercapnia according to the included AECOPD population, with hypercapnia, RR (0.69 [95% CI,0.33 to 1.44], P=0.317), without hypercapnia, RR (2.61 [95% CI,1.41 to 4.83], P=0.002). Mortality, RR (0.92 [95% CI,0.56 to 1.52], P = 0.752). ICU length of stay, MD (-0.44 [95% CI,-1.01 to 0.13], P = 0.132). Complication rate, RR (0.22 [95% CI,0.13 to 0.39], P = 0.000). After subgroup analysis, the reintubation rate of HFNC and NIV has no statistical difference in patients with hypercapnia, but NIV can significantly reduce the reintubation rate in patients without hypercapnia. In the outcome measures of complication rate, HFNC significantly reduced complication rate compared with NIV. In mortality and ICU length of stay, analysis results showed that HFNC and NIV were not statistically different.
Conclusion: According to the available evidence, the application of HFNC can be used as an alternative treatment for NIV after extubation in AECOPD patients with hypercapnia, but in the patients without hypercapnia, HFNC is less effective than NIV.
Keywords: acute exacerbation of chronic obstructive pulmonary disease; meta-analysis; nasal high-flow oxygen therapy; non-invasive ventilation.
© 2022 Feng et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
References
-
- Augusti A, Beasley R, Celli BR, et al. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnoses, management, and prevention of COPD; 2020. Available from: http://www.goldcopd.org. Accessed May 27, 2021.
-
- Osadnik CR, Tee VS, Carson-Chahhoud KV, Picot J, Wedzicha JA, Smith BJ. Non-invasive ventilation for the management of acute hypercapnic respiratory failure due to exacerbation of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2017;7(7):CD004104. doi: 10.1002/14651858.CD004104.pub4 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
