

Diabetes Mellitus and the Benefit of Antiresorptive Therapy on Fracture Risk
- PMID: 36065588
- PMCID: PMC10092457
- DOI: 10.1002/jbmr.4697
Diabetes Mellitus and the Benefit of Antiresorptive Therapy on Fracture Risk
Abstract
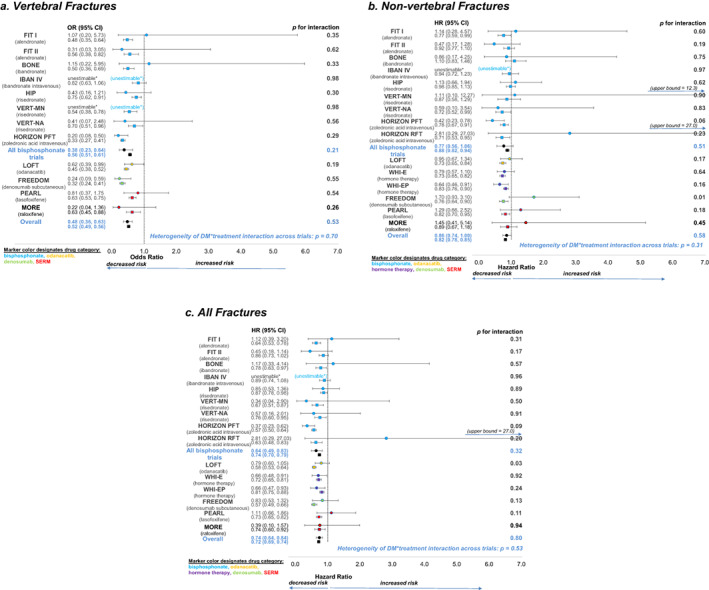
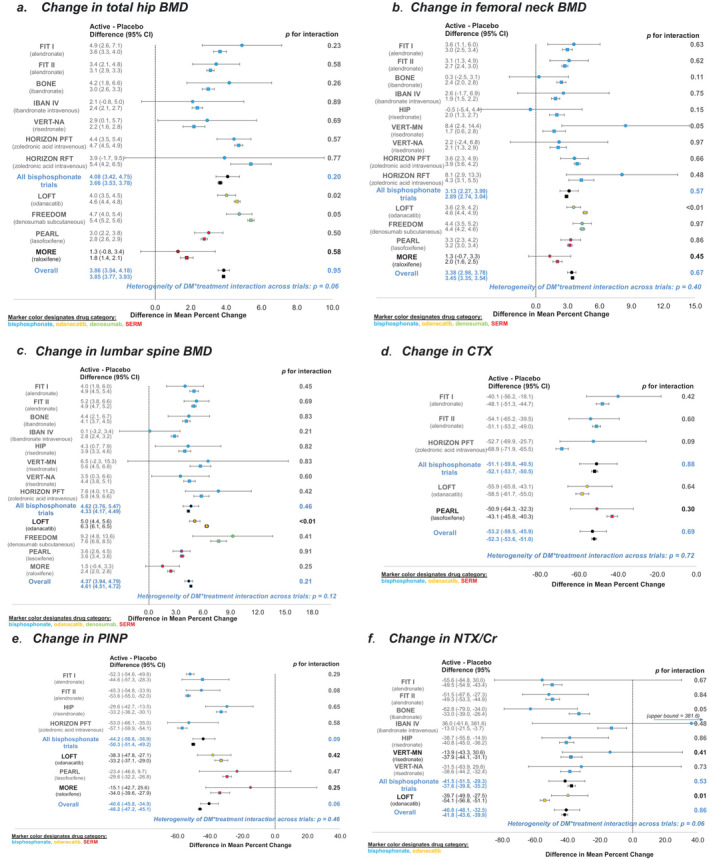
Type 2 diabetes (T2D) is associated with increased risk of fractures. However, it is unclear whether current osteoporosis treatments reduce fractures in individuals with diabetes. The aim of the study was to determine whether presence of T2D influences the efficacy of antiresorptive treatment for osteoporosis using the Foundation for the National Institutes of Health (FNIH)-American Society for Bone and Mineral Research (ASBMR)-Study to Advance Bone Mineral Density (BMD) as a Regulatory Endpoint (SABRE) cohort, which includes individual patient data from randomized trials of osteoporosis therapies. In this study we included 96,385 subjects, 6.8% of whom had T2D, from nine bisphosphonate trials, two selective estrogen receptor modulator (SERM) trials, two trials of menopausal hormone therapy, one denosumab trial, and one odanacatib trial. We used Cox regression to obtain the treatment hazard ratio (HR) for incident nonvertebral, hip, and all fractures and logistic regression to obtain the treatment odds ratio (OR) for incident morphometric vertebral fractures, separately for T2D and non-DM. We used linear regression to estimate the effect of treatment on 2-year change in BMD (n = 49,099) and 3-month to 12-month change in bone turnover markers (n = 12,701) by diabetes status. In all analyses, we assessed the interaction between treatment and diabetes status. In pooled analyses of all 15 trials, we found that diabetes did not impact treatment efficacy, with similar reductions in vertebral, nonvertebral, all, and hip fractures, increases in total hip and femoral neck BMD, and reductions in serum C-terminal cross-linking telopeptide (CTX), urinary N-telopeptide of type I collagen/creatinine (NTX/Cr) and procollagen type 1 N propeptide (P1NP) (all interactions p > 0.05). We found similar results for the pooled analysis of bisphosphonate trials. However, when we considered trials individually, we found a few interactions within individual studies between diabetes status and the effects of denosumab and odanacatib on fracture risk, change in BMD or bone turnover markers (BTMs). In sum, these results provide strong evidence that bisphosphonates and most licensed antiresorptive drugs are effective at reducing fracture risk and increasing BMD irrespective of diabetes status. © 2022 The Authors. Journal of Bone and Mineral Research published by Wiley Periodicals LLC on behalf of American Society for Bone and Mineral Research (ASBMR).
Keywords: ANTIRESORPTIVES; BIOCHEMICAL MARKERS OF BONE REMODELING; CLINICAL TRIALS; DXA; OSTEOPOROSIS.
© 2022 The Authors. Journal of Bone and Mineral Research published by Wiley Periodicals LLC on behalf of American Society for Bone and Mineral Research (ASBMR).
Conflict of interest statement
RE: reports grants from Amgen, grants and personal fees from Immunodiagnostic Systems, grants from Alexion, grants and personal fees from Roche, personal fees from Eli Lilly, personal fees from GSK Nutrition, personal fees from Mereo, personal fees from Sandoz, grants and personal fees from Nittobo, personal fees from AbbVie, personal fees from Samsung, personal fees from Haoma Medica, personal fees from Elsevier, personal fees from CL Bio, personal fees from FNIH, personal fees from Viking, outside the submitted work. EV: reports salary support from FNIH, during the conduct of the study. DMB: personal fees from Merck, personal fees from Amgen, personal fees from Asahi‐Kasei, personal fees from Effx, during the conduct of the study; personal fees from Eli Lilly, personal fees from University of Pittsburgh, outside the submitted work. MLB: received a grant from the Foundation for the NIH in relation to the submitted work, and grants from Amgen and Radius Pharma unrelated to this work; personal fees from Beryl Health, Agnovos and Keros Therapeutics. LYL, SKE, DCB, and AVS have nothing to disclose.
Figures
References
-
- Vilaca T, Schini M, Harnan S, et al. The risk of hip and non‐vertebral fractures in type 1 and type 2 diabetes: a systematic review and meta‐analysis update. Bone. 2020;137:115457. - PubMed
-
- Vestergaard P. Discrepancies in bone mineral density and fracture risk in patients with type 1 and type 2 diabetes—a meta‐analysis. Osteoporos Int. 2007;18(4):427‐444. - PubMed
-
- Hygum K, Starup‐Linde J, Harslof T, Vestergaard P, Langdahl BL. Mechanisms in endocrinology: diabetes mellitus, a state of low bone turnover—a systematic review and meta‐analysis. Eur J Endocrinol. 2017;176(3):R137‐R157. - PubMed
-
- Keegan TH, Schwartz AV, Bauer DC, Sellmeyer DE, Kelsey JL. Effect of alendronate on bone mineral density and biochemical markers of bone turnover in type 2 diabetic women: the fracture intervention trial. Diabetes Care. 2004;27(7):1547‐1553. - PubMed
-
- Johnell O, Kanis JA, Black DM, et al. Associations between baseline risk factors and vertebral fracture risk in the Multiple Outcomes of Raloxifene Evaluation (MORE) study. J Bone Miner Res. 2004;19(5):764‐772. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
