

Myocarditis following COVID-19 vaccine: incidence, presentation, diagnosis, pathophysiology, therapy, and outcomes put into perspective. A clinical consensus document supported by the Heart Failure Association of the European Society of Cardiology (ESC) and the ESC Working Group on Myocardial and Pericardial Diseases
- PMID: 36065751
- PMCID: PMC9538893
- DOI: 10.1002/ejhf.2669
Myocarditis following COVID-19 vaccine: incidence, presentation, diagnosis, pathophysiology, therapy, and outcomes put into perspective. A clinical consensus document supported by the Heart Failure Association of the European Society of Cardiology (ESC) and the ESC Working Group on Myocardial and Pericardial Diseases
Erratum in
-
Corrigendum to: 'A comprehensive characterization of acute heart failure with preserved versus mildly reduced versus reduced ejection fraction - insights from the ESC-HFA EORP Heart Failure Long-Term Registry' and articles listed below.Eur J Heart Fail. 2023 Mar;25(3):443. doi: 10.1002/ejhf.2789. Epub 2023 Feb 17. Eur J Heart Fail. 2023. PMID: 36799232 Free PMC article. No abstract available.
Abstract
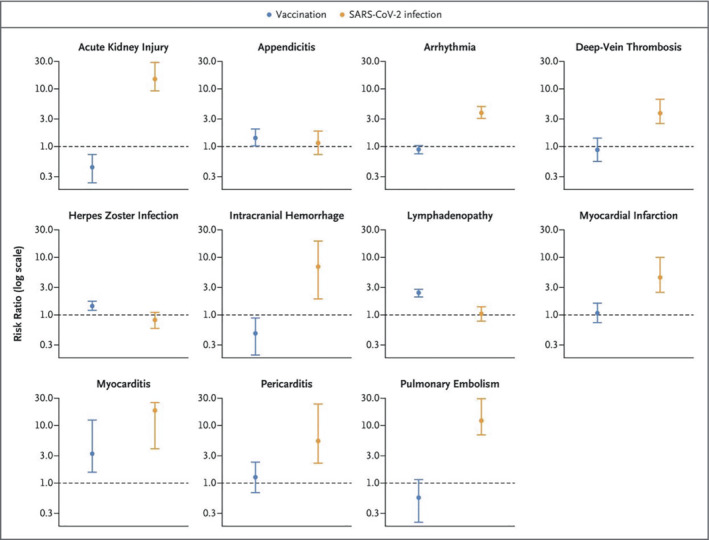
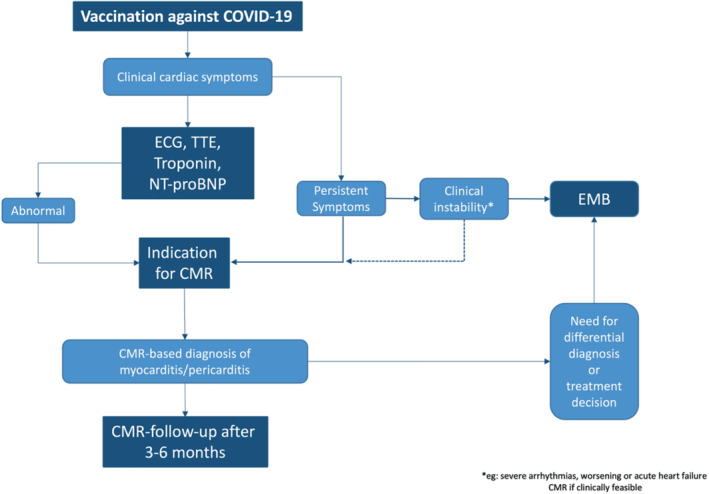
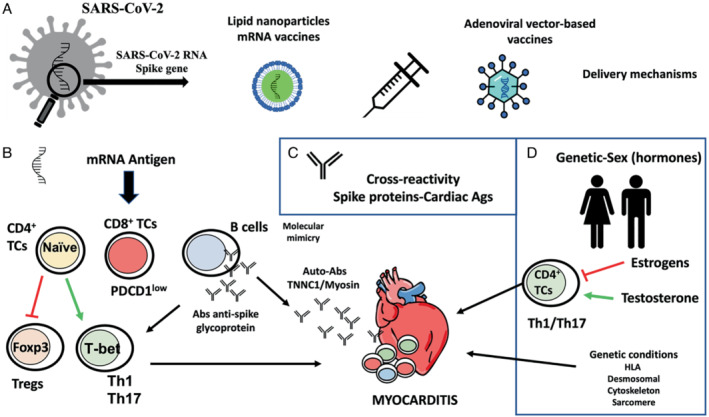
Over 10 million doses of COVID-19 vaccines based on RNA technology, viral vectors, recombinant protein, and inactivated virus have been administered worldwide. Although generally very safe, post-vaccine myocarditis can result from adaptive humoral and cellular, cardiac-specific inflammation within days and weeks of vaccination. Rates of vaccine-associated myocarditis vary by age and sex with the highest rates in males between 12 and 39 years. The clinical course is generally mild with rare cases of left ventricular dysfunction, heart failure and arrhythmias. Mild cases are likely underdiagnosed as cardiac magnetic resonance imaging (CMR) is not commonly performed even in suspected cases and not at all in asymptomatic and mildly symptomatic patients. Hospitalization of symptomatic patients with electrocardiographic changes and increased plasma troponin levels is considered necessary in the acute phase to monitor for arrhythmias and potential decline in left ventricular function. In addition to evaluation for symptoms, electrocardiographic changes and elevated troponin levels, CMR is the best non-invasive diagnostic tool with endomyocardial biopsy being restricted to severe cases with heart failure and/or arrhythmias. The management beyond guideline-directed treatment of heart failure and arrhythmias includes non-specific measures to control pain. Anti-inflammatory drugs such as non-steroidal anti-inflammatory drugs, and corticosteroids have been used in more severe cases, with only anecdotal evidence for their effectiveness. In all age groups studied, the overall risks of SARS-CoV-2 infection-related hospitalization and death are hugely greater than the risks from post-vaccine myocarditis. This consensus statement serves as a practical resource for physicians in their clinical practice, to understand, diagnose, and manage affected patients. Furthermore, it is intended to stimulate research in this area.
Keywords: COVID-19; Inflammation; Myocarditis; Outcomes; Pathology; Vaccination.
© 2022 The Authors. European Journal of Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Figures
References
-
- Johns Hopkins Corona Virus Resource Center . COVID‐19 Dashboard. https://coronavirus.jhu.edu/map.html (last accessed 8 September 2022).
-
- Shay DK, Shimabukuro TT, DeStefano F. Myocarditis occurring after immunization with mRNA‐based COVID‐19 vaccines. JAMA Cardiol. 6:1115–7. - PubMed
-
- Shiyovich A, Witberg G, Aviv Y, Eisen A, Orvin K, Wiessman M, et al. Myocarditis following COVID‐19 vaccination: magnetic resonance imaging study. Eur Heart J Cardiovasc Imaging. 2021;23:1075–82. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
