

Association Between Time to Appropriate Antimicrobial Treatment and 30-day Mortality in Patients With Bloodstream Infections: A Retrospective Cohort Study
- PMID: 36065752
- PMCID: PMC9907509
- DOI: 10.1093/cid/ciac727
Association Between Time to Appropriate Antimicrobial Treatment and 30-day Mortality in Patients With Bloodstream Infections: A Retrospective Cohort Study
Abstract
Background: Effective antimicrobial treatment is key for survival in bloodstream infection (BSI), but the impact of timing of treatment remains unclear. Our aim was to assess the association between time to appropriate antimicrobial treatment and 30-day mortality in BSI patients.
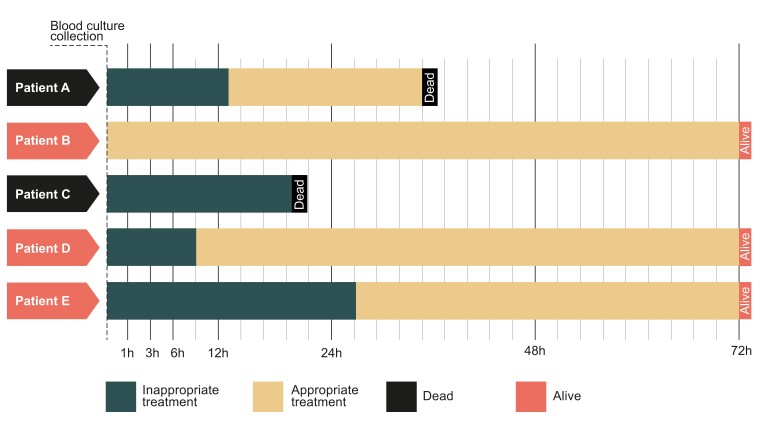
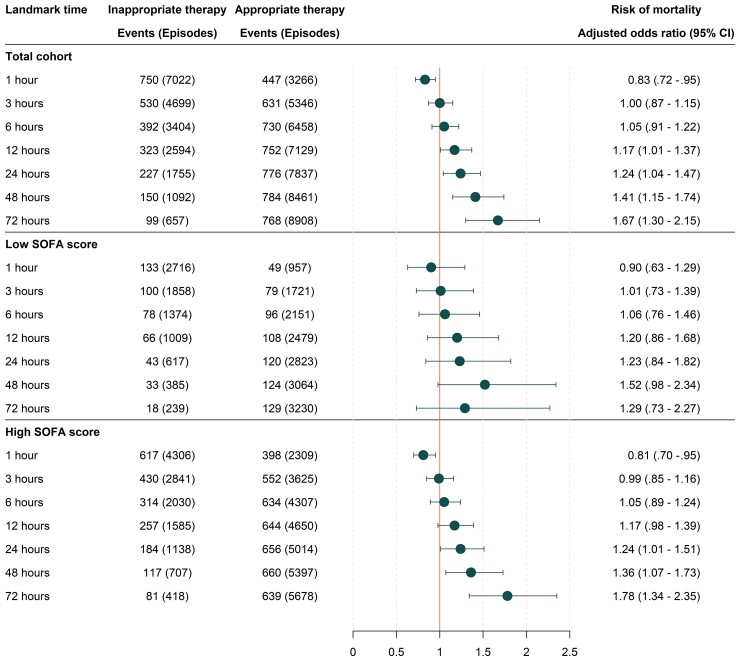
Methods: This was a retrospective cohort study using electronic health record data from a large academic center in Sweden. Adult patients admitted between the years 2012 and 2019, with onset of BSI at the emergency department or general wards, were included. Pathogen-antimicrobial drug combinations were classified as appropriate or inappropriate based on reported in vitro susceptibilities. To avoid immortal time bias, the association between appropriate therapy and mortality was assessed with multivariable logistic regression analysis at pre-specified landmark times.
Results: We included 10 628 BSI-episodes, occurring in 9192 unique patients. The overall 30-day mortality was 11.8%. No association in favor of a protective effect between appropriate therapy and mortality was found at the 1, 3 and 6 hours landmark after blood culture collection. At 12 hours, the risk of death increased with inappropriate treatment (adjusted odds ratio 1.17 [95% confidence interval {CI}, 1.01-1.37]) and continued to increase gradually at 24, 48, and 72 hours. Stratifying by high or low SOFA score generated similar odds ratios, with wider confidence intervals.
Conclusions: Delays in appropriate antimicrobial treatment were associated with increased 30-day mortality after 12 hours from blood culture collection, but not at 1, 3, and 6 hours, in BSI. These results indicate a benchmark for providing rapid microbiological diagnostics of blood cultures.
Keywords: antimicrobial treatment; bloodstream infection; mortality.
© The Author(s) 2022. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest . J. V. H. reports support for attending meetings and/or travel from ESCMID (ESCMID Young Scientist travel grant for poster presentation at ECCMID 2022). All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures

References
-
- Laupland KB, Lyytikäinen O, Søgaard M, et al. The changing epidemiology of Staphylococcus aureus bloodstream infection: a multinational population-based surveillance study. Clin Microbiol Infect 2013; 19:465–71. - PubMed
-
- Leibovici L, Paul M, Ezra O. Ethical dilemmas in antibiotic treatment. J Antimicrob Chemother 2012; 67:12–6. - PubMed
-
- Friedman ND, Temkin E, Carmeli Y. The negative impact of antibiotic resistance. Clin Microbiol Infect 2016; 22:416–22. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
