

Liver and spleen volumes are associated with prognosis of compensated and decompensated cirrhosis and parallel its natural history
- PMID: 36065767
- PMCID: PMC9557954
- DOI: 10.1002/ueg2.12301
Liver and spleen volumes are associated with prognosis of compensated and decompensated cirrhosis and parallel its natural history
Abstract
Objective: Cirrhosis is characterized by the complex interplay among biological, histological and haemodynamic events. Liver and spleen remodelling occur throughout its natural history, but the prognostic role of these volumetric changes is unclear. We evaluated the relationship between volumetric changes assessed by multidetector computerised tomography (MDCT) and landmark features of cirrhosis.
Methods: We included consecutive cirrhotic patients who underwent liver transplantation (LT) or hepatocellular carcinoma (HCC) resection in whom dynamic MDCT was available. Different volumetric indices were calculated. Fibrosis was evaluated by the collagen proportional area and Laennec sub-stages. Correlation and logistic regression analysis were performed to explore associations of volumetric indexes and fibrosis with key prognostic features across the clinical stages of cirrhosis.
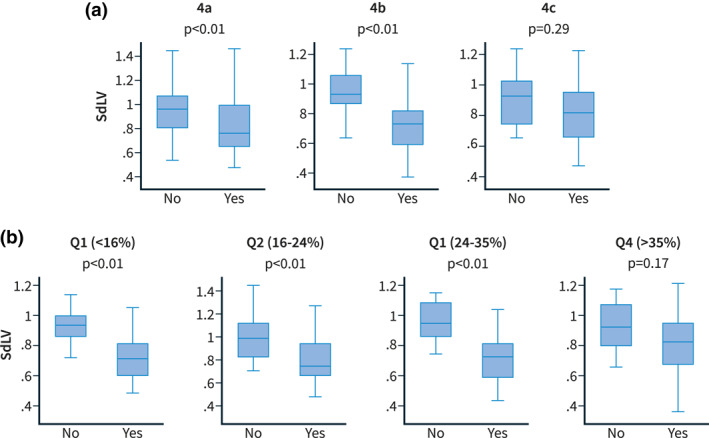
Results: 185 patients were included (146 LT; 39 HCC); the predominant aetiology was viral hepatitis (51.35%); 65.9% had decompensated disease and 85.08% clinically significant portal hypertension (CSPH). The standardised liver volume and liver-spleen volume ratio negatively correlated with Model for End-stage Liver Disease (MELD), albumin and hepatic venous pressure gradient (HVPG) and were significantly lower in decompensated patients. The liver segmental volume ratio (segments I-III/segments IV-VIII) best captured the characteristic features of the compensated phase, showing a positive correlation with HVPG and a good discrimination between patients with and without CSPH and varices. Volumetric changes and fibrosis severity were independently associated with key prognostic events, with no association between these two parameters.
Conclusions: Liver and spleen volumetric indices evolve differently along the natural history of cirrhosis and are associated with key prognostic factors in each phase, regardless of fibrosis severity and portal hypertension.
Keywords: cirrhosis; fibrosis; natural history; portal hypertension; tomography.
© 2022 The Authors. United European Gastroenterology Journal published by Wiley Periodicals LLC. on behalf of United European Gastroenterology.
Conflict of interest statement
No conflict of interest to declare.
Figures




Comment in
-
Can we predict the future of patients with liver cirrhosis using volumetrics?United European Gastroenterol J. 2022 Oct;10(8):791-792. doi: 10.1002/ueg2.12308. Epub 2022 Sep 12. United European Gastroenterol J. 2022. PMID: 36094879 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
