

Pregnancy and infant outcomes by trimester of SARS-CoV-2 infection in pregnancy-SET-NET, 22 jurisdictions, January 25, 2020-December 31, 2020
- PMID: 36065896
- PMCID: PMC9537929
- DOI: 10.1002/bdr2.2081
Pregnancy and infant outcomes by trimester of SARS-CoV-2 infection in pregnancy-SET-NET, 22 jurisdictions, January 25, 2020-December 31, 2020
Abstract
Objectives: We describe clinical characteristics, pregnancy, and infant outcomes in pregnant people with laboratory-confirmed SARS-CoV-2 infection by trimester of infection.
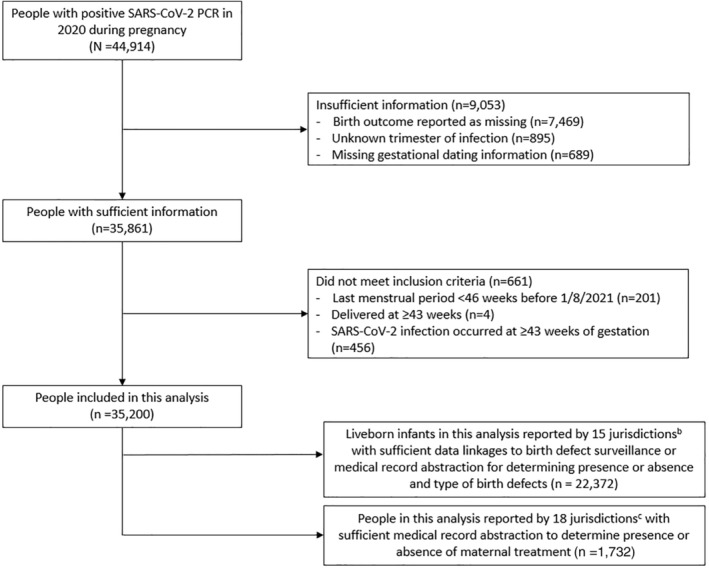
Study design: We analyzed data from the Surveillance for Emerging Threats to Mothers and Babies Network and included people with infection in 2020, with known timing of infection and pregnancy outcome. Outcomes are described by trimester of infection. Pregnancy outcomes included live birth and pregnancy loss (<20 weeks and ≥20 weeks gestation). Infant outcomes included preterm birth (<37 weeks gestation), small for gestational age, birth defects, and neonatal intensive care unit admission. Adjusted prevalence ratios (aPR) were calculated for pregnancy and selected infant outcomes by trimester of infection, controlling for demographics.
Results: Of 35,200 people included in this analysis, 50.8% of pregnant people had infection in the third trimester, 30.8% in the second, and 18.3% in the first. Third trimester infection was associated with a higher frequency of preterm birth compared to first or second trimester infection combined (17.8% vs. 11.8%; aPR 1.44 95% CI: 1.35-1.54). Prevalence of birth defects was 553.4/10,000 live births, with no difference by trimester of infection.
Conclusions: There were no signals for increased birth defects among infants in this population relative to national baseline estimates, regardless of timing of infection. However, the prevalence of preterm birth in people with SARS-CoV-2 infection in pregnancy in our analysis was higher relative to national baseline data (10.0-10.2%), particularly among people with third trimester infection. Consequences of COVID-19 during pregnancy support recommended COVID-19 prevention strategies, including vaccination.
Keywords: COVID-19; SARS-CoV-2; pregnancy.
Published 2022. This article is a U.S. Government work and is in the public domain in the USA.
Conflict of interest statement
All authors have no conflicts of interest to disclose.
Figures
References
-
- 45 C.F.R. part 46 , 21 C.F.R. part 56; 42 U.S.C. Sect. 241(d); 5 U.S.C. Sect. 552a; 44 U.S.C. Sect. 3501 et seq, 2018.
-
- Allotey, J. , Chatterjee, S. , Kew, T. , Gaetano, A., Stallings, E., Fernandez‐Garcia, S., … Thangaratinam, S. (2022). SARS‐CoV‐2 positivity in offspring and timing of mother‐to‐child transmission: Living systematic review and meta‐analysis. BMJ, 376, e067696. 10.1136/bmj-2021-067696 - DOI - PMC - PubMed
-
- Allotey, J. , Stallings, E. , Bonet, M. , Yap, M., Chatterjee, S., Kew, T., … Thangaratinam, S. (2020). Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: Living systematic review and meta‐analysis. BMJ, 370, m3320. 10.1136/bmj.m3320 - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
