

Bronchodilators in Tobacco-Exposed Persons with Symptoms and Preserved Lung Function
- PMID: 36066078
- PMCID: PMC9741866
- DOI: 10.1056/NEJMoa2204752
Bronchodilators in Tobacco-Exposed Persons with Symptoms and Preserved Lung Function
Abstract
Background: Many persons with a history of smoking tobacco have clinically significant respiratory symptoms despite an absence of airflow obstruction as assessed by spirometry. They are often treated with medications for chronic obstructive pulmonary disease (COPD), but supporting evidence for this treatment is lacking.
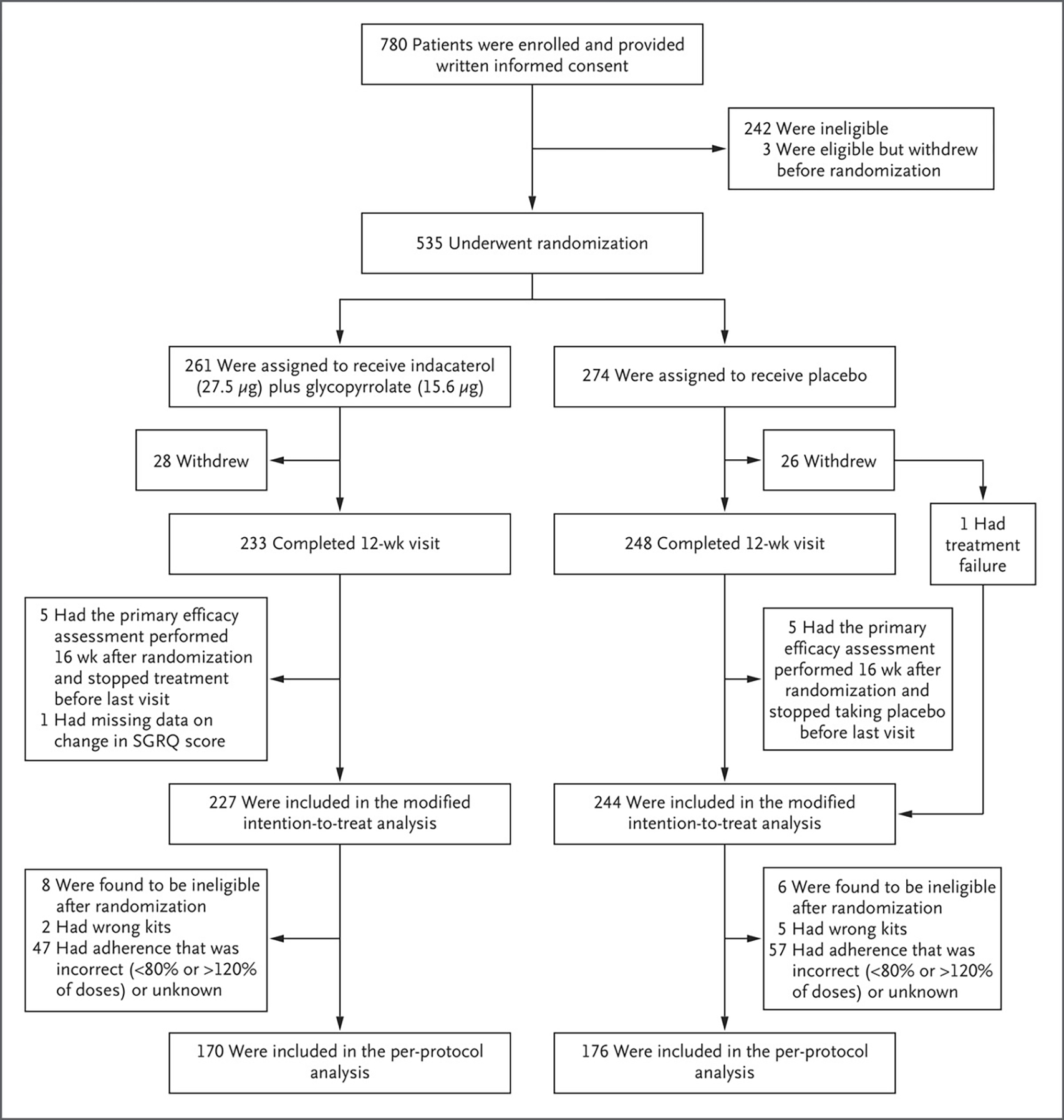
Methods: We randomly assigned persons who had a tobacco-smoking history of at least 10 pack-years, respiratory symptoms as defined by a COPD Assessment Test score of at least 10 (scores range from 0 to 40, with higher scores indicating worse symptoms), and preserved lung function on spirometry (ratio of forced expiratory volume in 1 second [FEV1] to forced vital capacity [FVC] ≥0.70 and FVC ≥70% of the predicted value after bronchodilator use) to receive either indacaterol (27.5 μg) plus glycopyrrolate (15.6 μg) or placebo twice daily for 12 weeks. The primary outcome was at least a 4-point decrease (i.e., improvement) in the St. George's Respiratory Questionnaire (SGRQ) score (scores range from 0 to 100, with higher scores indicating worse health status) after 12 weeks without treatment failure (defined as an increase in lower respiratory symptoms treated with a long-acting inhaled bronchodilator, glucocorticoid, or antibiotic agent).
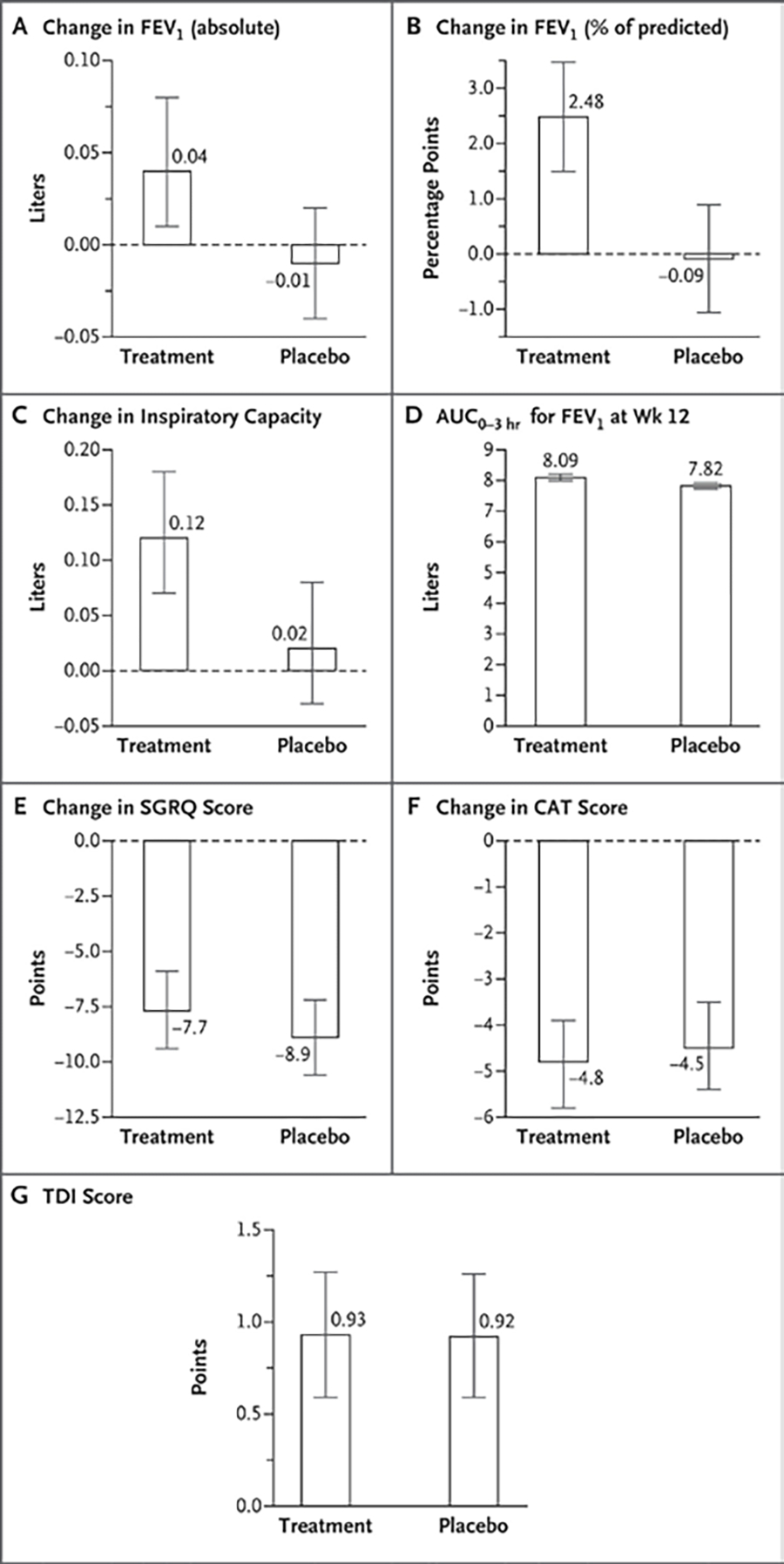
Results: A total of 535 participants underwent randomization. In the modified intention-to-treat population (471 participants), 128 of 227 participants (56.4%) in the treatment group and 144 of 244 (59.0%) in the placebo group had at least a 4-point decrease in the SGRQ score (difference, -2.6 percentage points; 95% confidence interval [CI], -11.6 to 6.3; adjusted odds ratio, 0.91; 95% CI, 0.60 to 1.37; P = 0.65). The mean change in the percent of predicted FEV1 was 2.48 percentage points (95% CI, 1.49 to 3.47) in the treatment group and -0.09 percentage points (95% CI, -1.06 to 0.89) in the placebo group, and the mean change in the inspiratory capacity was 0.12 liters (95% CI, 0.07 to 0.18) in the treatment group and 0.02 liters (95% CI, -0.03 to 0.08) in the placebo group. Four serious adverse events occurred in the treatment group, and 11 occurred in the placebo group; none were deemed potentially related to the treatment or placebo.
Conclusions: Inhaled dual bronchodilator therapy did not decrease respiratory symptoms in symptomatic, tobacco-exposed persons with preserved lung function as assessed by spirometry. (Funded by the National Heart, Lung, and Blood Institute and others; RETHINC ClinicalTrials.gov number, NCT02867761.).
Copyright © 2022 Massachusetts Medical Society.
Figures

Comment in
-
RETHINCking COPD - Bronchodilators for Symptomatic Tobacco-Exposed Persons with Preserved Lung Function?N Engl J Med. 2022 Sep 29;387(13):1230-1231. doi: 10.1056/NEJMe2210347. Epub 2022 Sep 4. N Engl J Med. 2022. PMID: 36066080 No abstract available.
-
Bronchodilatation hilft Rauchern nur bei gesicherter COPD.MMW Fortschr Med. 2022 Nov;164(20):30-31. doi: 10.1007/s15006-022-2092-4. MMW Fortschr Med. 2022. PMID: 36376668 German. No abstract available.
-
In tobacco smokers with respiratory symptoms, a dual bronchodilator did not reduce symptoms at 12 wk.Ann Intern Med. 2023 Jan;176(1):JC6. doi: 10.7326/J22-0103. Epub 2023 Jan 3. Ann Intern Med. 2023. PMID: 36592470
References
-
- Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med 2017;195:557–82. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U01 HL128952/HL/NHLBI NIH HHS/United States
- P30 ES005605/ES/NIEHS NIH HHS/United States
- K24 HL140108/HL/NHLBI NIH HHS/United States
- UL1 TR001422/TR/NCATS NIH HHS/United States
- U01 HL137880/HL/NHLBI NIH HHS/United States
- HL128954/HL/NHLBI NIH HHS/United States
- U01 HL128954/HL/NHLBI NIH HHS/United States
- KL2 TR001882/TR/NCATS NIH HHS/United States
- HL128952/HL/NHLBI NIH HHS/United States
- K24 HL138188/HL/NHLBI NIH HHS/United States
- I01 CX001048/CX/CSRD VA/United States
- K24 HL137013/HL/NHLBI NIH HHS/United States
- I01 CX000105/CX/CSRD VA/United States
- UL1 TR002384/TR/NCATS NIH HHS/United States
- P30 CA014236/CA/NCI NIH HHS/United States
- R01 HL149719/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical