

Operative Time is Associated With Postoperative Complications After Pulmonary Lobectomy
- PMID: 36066195
- PMCID: PMC9985664
- DOI: 10.1097/SLA.0000000000005696
Operative Time is Associated With Postoperative Complications After Pulmonary Lobectomy
Abstract
Objective: To investigate the association between operative time and postoperative outcomes.
Background: The association between operative time and morbidity after pulmonary lobectomy has not been characterized fully.
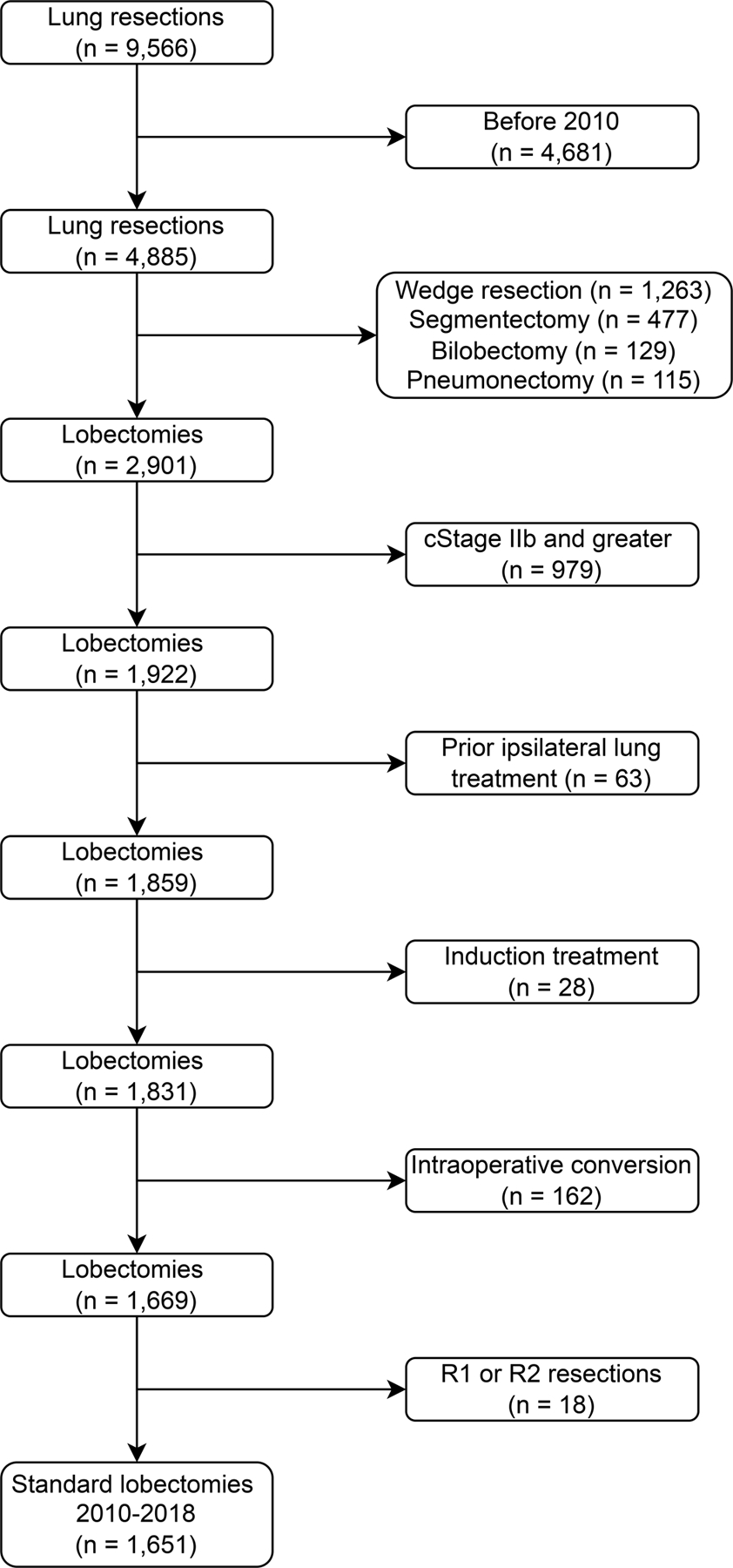
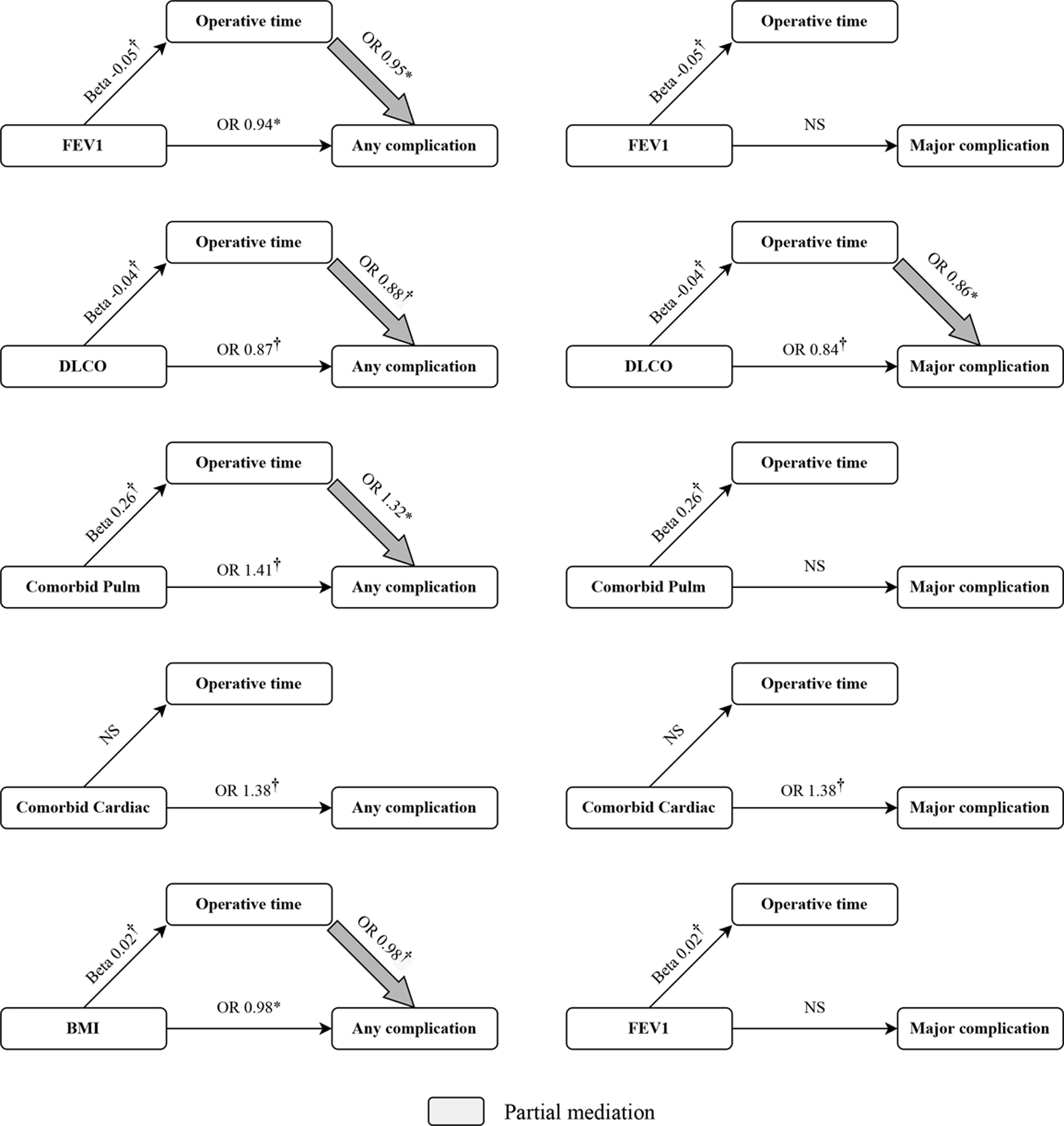
Methods: Patients who underwent pulmonary lobectomy for primary lung cancer at our institution from 2010 to 2018 were reviewed. Exclusion criteria included clinical stage ≥IIb disease, conversion to thoracotomy, and previous ipsilateral lung treatment. Operative time was measured from incision to closure. Relationships between operative time and outcomes were quantified using multivariable mixed-effects models with surgeon-level random effects.
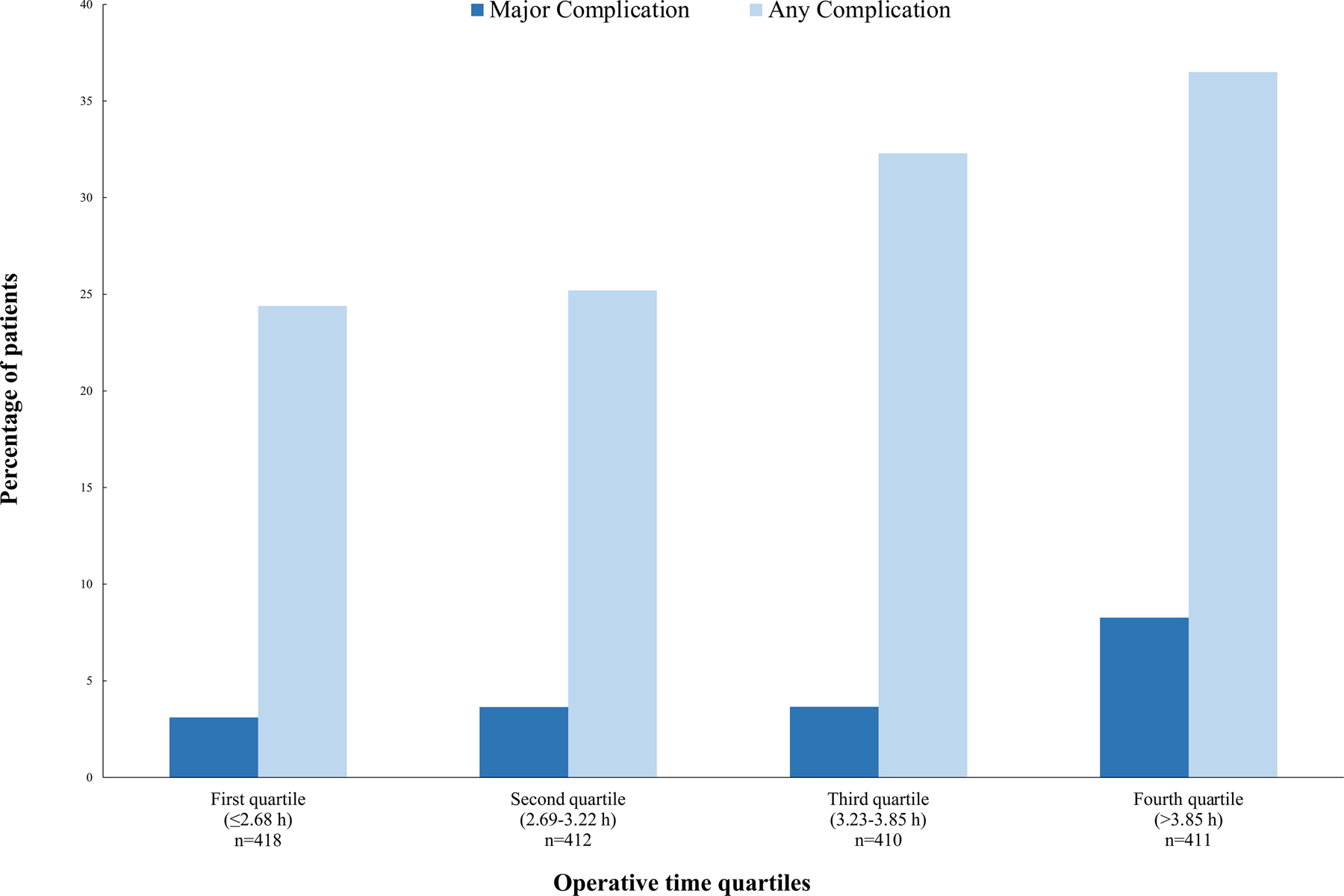
Results: In total, 1651 patients were included. The median age was 68 years (interquartile range, 61-74), and 63% of patients were women. Median operative time was 3.2 hours (interquartile range, 2.7-3.8) for all cases, 3.0 hours for open procedures, 3.3 hours for video-assisted thoracoscopies, and 3.3 hours for robotic procedures ( P =0.0002). Overall, 488 patients (30%) experienced a complication; 77 patients (5%) had a major complication (grade ≥3), and 5 patients (0.3%) died within 30 days of discharge. On multivariable analysis, operative time was associated with higher odds of any complication [odds ratio per hour, 1.37; 95% confidence interval (CI), 1.20-1.57; P <0.0001] and major complication (odds ratio per hour, 1.41; 95% CI, 1.21-1.64; P <0.0001). Operative time was also associated with longer hospital length of stay (β, 1.09; 95% CI, 1.04-1.14; P =0.001).
Conclusions: Longer operative time was associated with worse outcomes in patients who underwent lobectomy. Operative time is a potential risk factor to consider in the perioperative phase.
Copyright © 2022 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Brunelli A, Dinesh P, Woodcock-Shaw J, et al. Ninety-day mortality after video-assisted thoracoscopic lobectomy: incidence and risk factors. Ann Thorac Surg. 2017;104:1020–1026. - PubMed
-
- Infante MV, Benato C, Silva R, et al. What counts more: the patient, the surgical technique, or the hospital? A multivariable analysis of factors affecting perioperative complications of pulmonary lobectomy by video-assisted thoracoscopic surgery from a large nationwide registry. Eur J Cardiothorac Surg. 2019;56:1097–1103. - PMC - PubMed
-
- Jean RA, DeLuzio MR, Kraev AI, et al. Analyzing risk factors for morbidity and mortality after lung resection for lung cancer using the NSQIP database. J Am Coll Surg. 2016;222:992–1000.e1. - PubMed
-
- Stéphan F, Boucheseiche S, Hollande J, et al. Pulmonary complications following lung resection. Chest. 2000;118:1263–1270. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
