

Consensus Recommendations for the Use of Automated Insulin Delivery Technologies in Clinical Practice
- PMID: 36066457
- PMCID: PMC9985411
- DOI: 10.1210/endrev/bnac022
Consensus Recommendations for the Use of Automated Insulin Delivery Technologies in Clinical Practice
Abstract
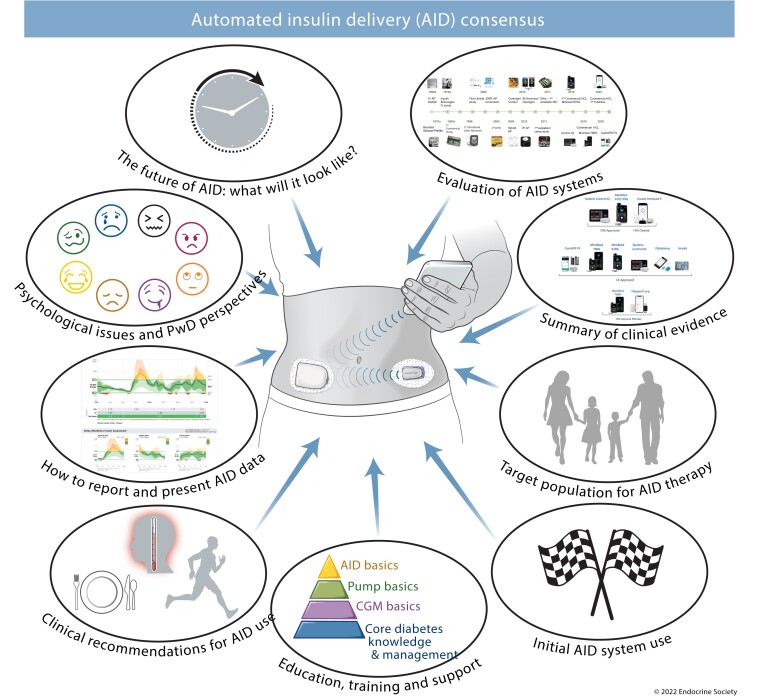
The significant and growing global prevalence of diabetes continues to challenge people with diabetes (PwD), healthcare providers, and payers. While maintaining near-normal glucose levels has been shown to prevent or delay the progression of the long-term complications of diabetes, a significant proportion of PwD are not attaining their glycemic goals. During the past 6 years, we have seen tremendous advances in automated insulin delivery (AID) technologies. Numerous randomized controlled trials and real-world studies have shown that the use of AID systems is safe and effective in helping PwD achieve their long-term glycemic goals while reducing hypoglycemia risk. Thus, AID systems have recently become an integral part of diabetes management. However, recommendations for using AID systems in clinical settings have been lacking. Such guided recommendations are critical for AID success and acceptance. All clinicians working with PwD need to become familiar with the available systems in order to eliminate disparities in diabetes quality of care. This report provides much-needed guidance for clinicians who are interested in utilizing AIDs and presents a comprehensive listing of the evidence payers should consider when determining eligibility criteria for AID insurance coverage.
Keywords: automated insulin delivery; closed-loop; consensus recommendations; type 1 diabetes.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Endocrine Society.
Figures

References
-
- McAuley SA, Lee MH, Paldus B, et al. Six months of hybrid closed-loop versus manual insulin delivery with fingerprick blood glucose monitoring in adults with type 1 diabetes: a randomized, controlled trial. Diabetes Care. 2020;43:3024–3033. - PubMed
-
- Collyns OJ, Meier RA, Betts ZL, et al. Improved glycemic outcomes with Medtronic MiniMed advanced hybrid closed-loop delivery: results from a randomized crossover trial comparing automated insulin delivery with predictive low glucose suspend in people with type 1 diabetes. Diabetes Care. 2021;44(4):969–975. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
