

Effect of an Individualized Audit and Feedback Intervention on Rates of Musculoskeletal Diagnostic Imaging Requests by Australian General Practitioners: A Randomized Clinical Trial
- PMID: 36066518
- PMCID: PMC9449798
- DOI: 10.1001/jama.2022.14587
Effect of an Individualized Audit and Feedback Intervention on Rates of Musculoskeletal Diagnostic Imaging Requests by Australian General Practitioners: A Randomized Clinical Trial
Abstract
Importance: Audit and feedback can improve professional practice, but few trials have evaluated its effectiveness in reducing potential overuse of musculoskeletal diagnostic imaging in general practice.
Objective: To evaluate the effectiveness of audit and feedback for reducing musculoskeletal imaging by high-requesting Australian general practitioners (GPs).
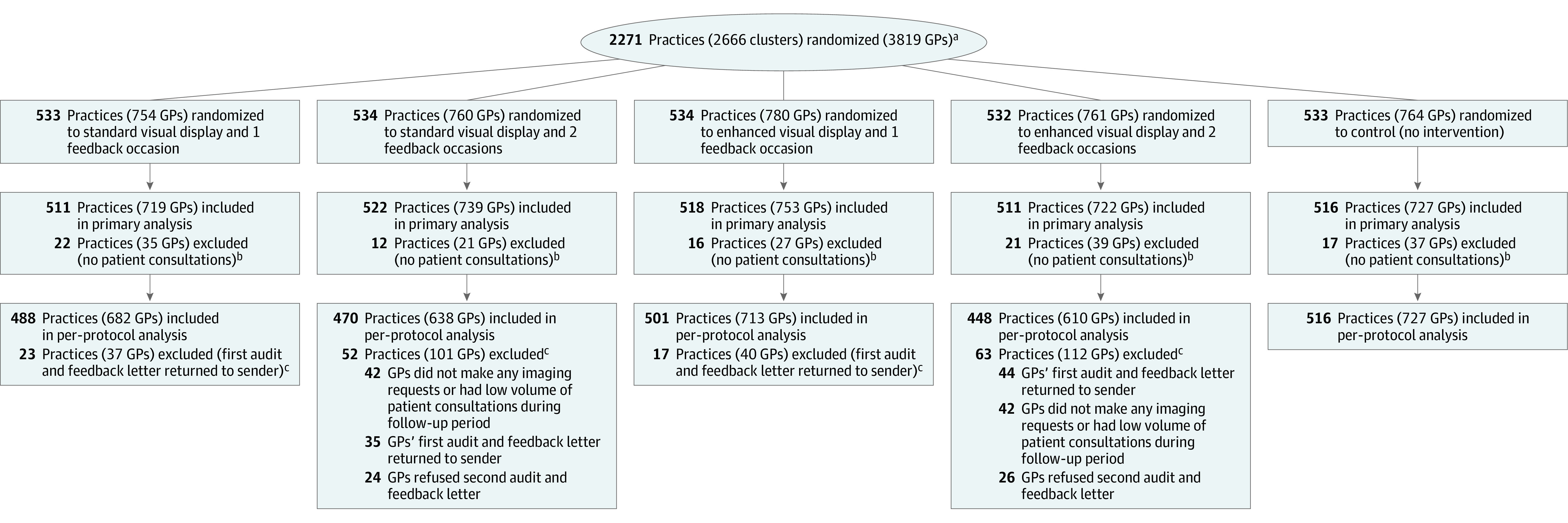
Design, setting, and participants: This factorial cluster-randomized clinical trial included 2271 general practices with at least 1 GP who was in the top 20% of referrers for 11 imaging tests (of the lumbosacral or cervical spine, shoulder, hip, knee, and ankle/hind foot) and for at least 4 individual tests between January and December 2018. Only high-requesting GPs within participating practices were included. The trial was conducted between November 2019 and May 2021, with final follow-up on May 8, 2021.
Interventions: Eligible practices were randomized in a 1:1:1:1:1 ratio to 1 of 4 different individualized written audit and feedback interventions (n = 3055 GPs) that varied factorially by (1) frequency of feedback (once vs twice) and (2) visual display (standard vs enhanced display highlighting highly requested tests) or to a control condition of no intervention (n = 764 GPs). Participants were not masked.
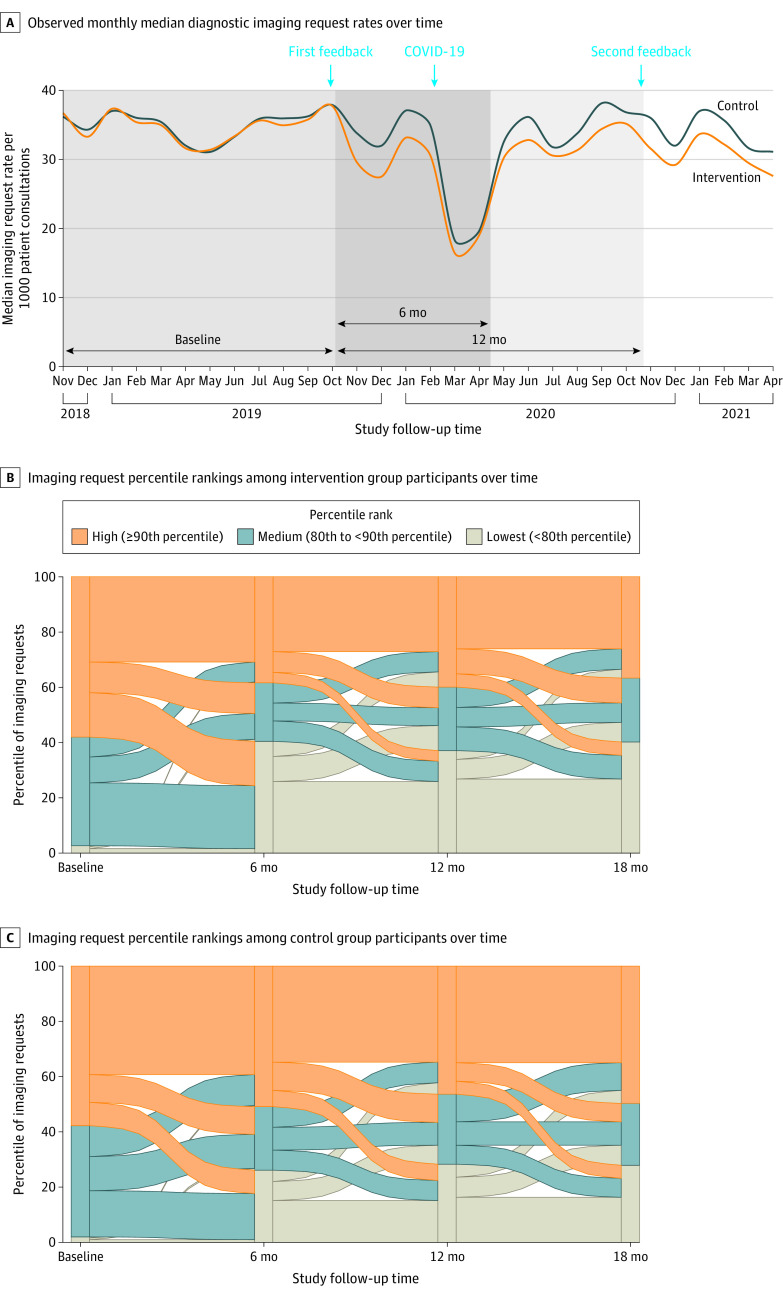
Main outcomes and measures: The primary outcome was the overall rate of requests for the 11 targeted imaging tests per 1000 patient consultations over 12 months, assessed using routinely collected administrative data. Primary analyses included all randomized GPs who had at least 1 patient consultation during the study period and were performed by statisticians masked to group allocation.
Results: A total of 3819 high-requesting GPs from 2271 practices were randomized, and 3660 GPs (95.8%; n = 727 control, n = 2933 intervention) were included in the primary analysis. Audit and feedback led to a statistically significant reduction in the overall rate of imaging requests per 1000 consultations compared with control over 12 months (adjusted mean, 27.7 [95% CI, 27.5-28.0] vs 30.4 [95% CI, 29.8-30.9], respectively; adjusted mean difference, -2.66 [95% CI, -3.24 to -2.07]; P < .001).
Conclusions and relevance: Among Australian general practitioners known to frequently request musculoskeletal diagnostic imaging, an individualized audit and feedback intervention, compared with no intervention, significantly decreased the rate of targeted musculoskeletal imaging tests ordered over 12 months.
Trial registration: ANZCTR Identifier: ACTRN12619001503112.
Conflict of interest statement
Figures
Comment in
-
Audit and Feedback-Optimizing a Strategy to Reduce Low-Value Care.JAMA. 2022 Sep 6;328(9):833-835. doi: 10.1001/jama.2022.14173. JAMA. 2022. PMID: 36066538 No abstract available.
-
Effect of an Individualized Audit and Feedback Intervention on Rates of Musculoskeletal Diagnostic Imaging Requests.JAMA. 2023 Jan 10;329(2):175. doi: 10.1001/jama.2022.20739. JAMA. 2023. PMID: 36625817 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
