

CD69 expression on regulatory T cells protects from immune damage after myocardial infarction
- PMID: 36066993
- PMCID: PMC9621142
- DOI: 10.1172/JCI152418
CD69 expression on regulatory T cells protects from immune damage after myocardial infarction
Abstract
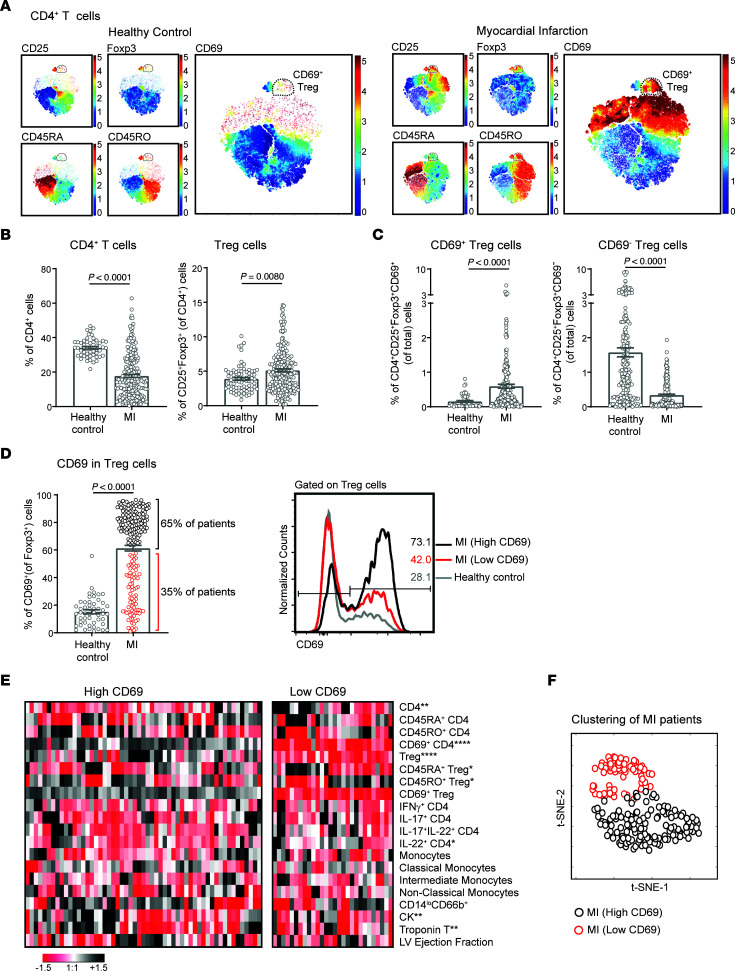
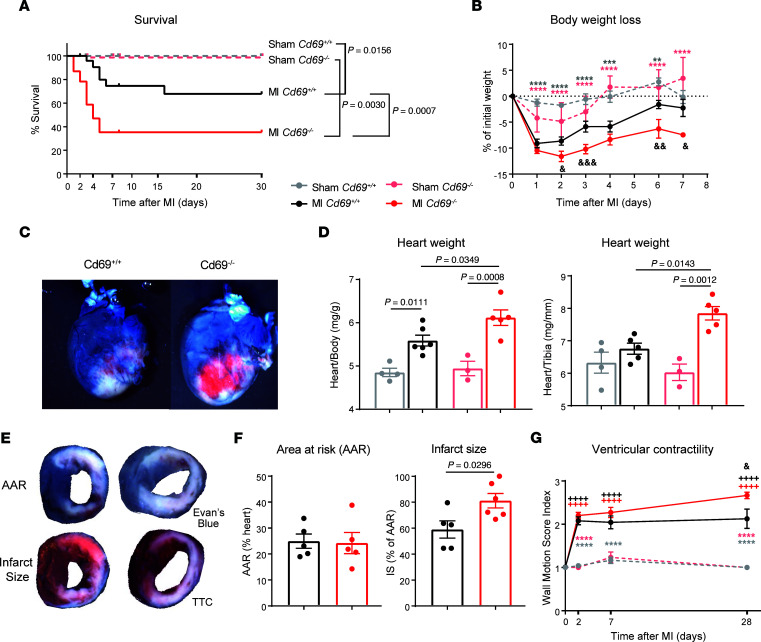
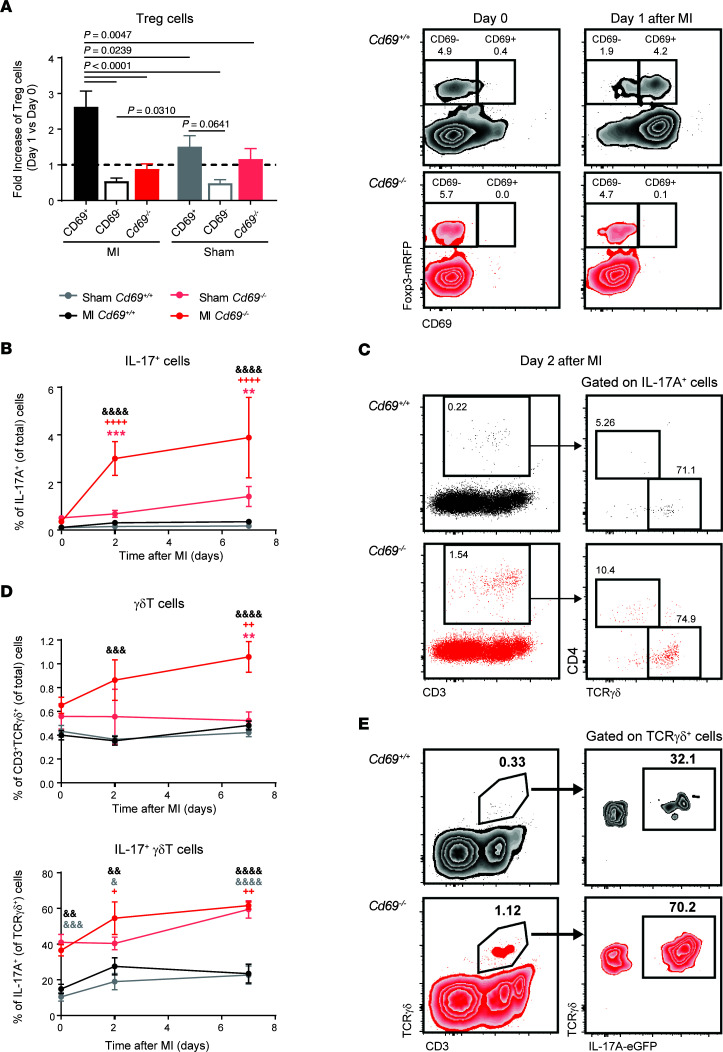
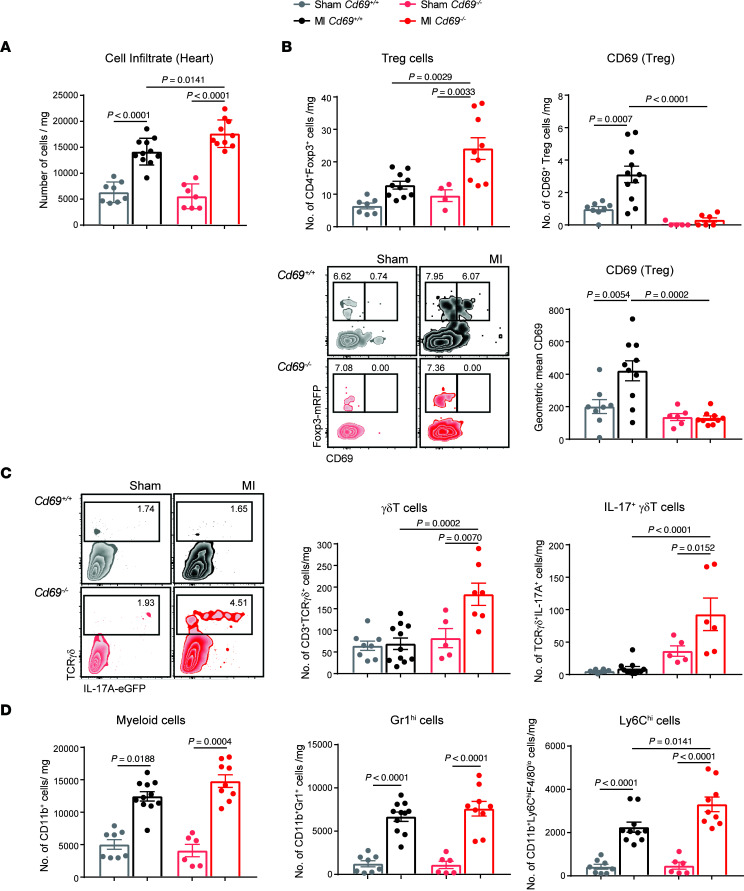
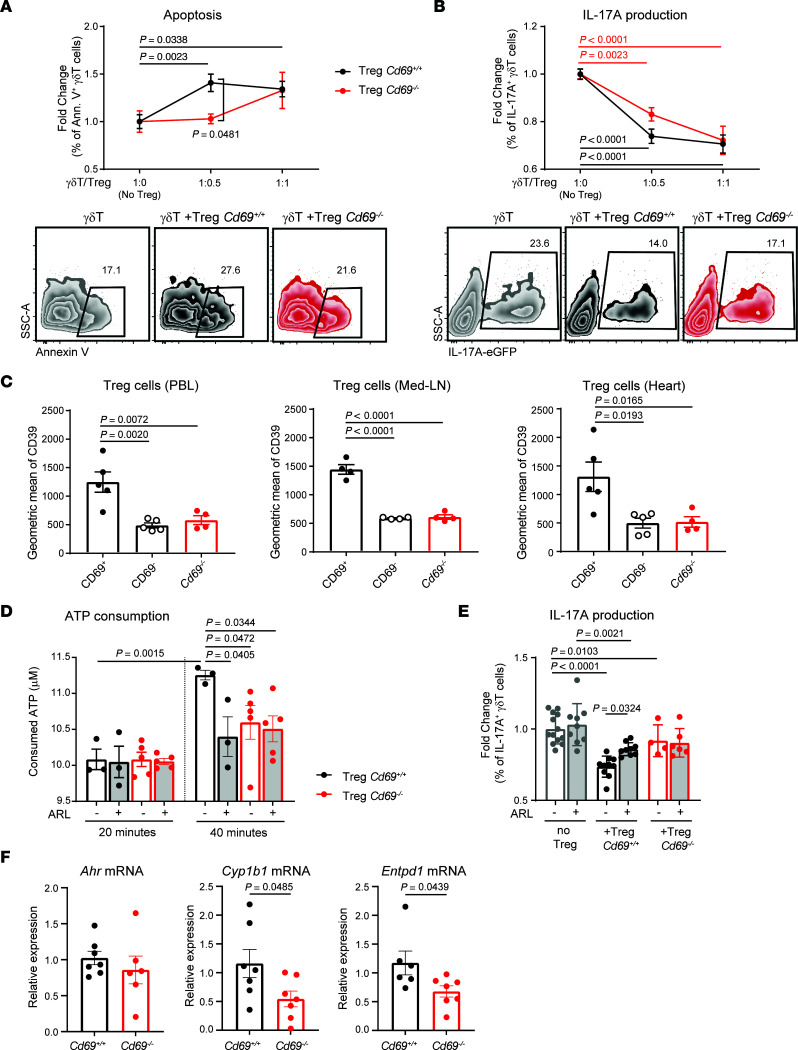
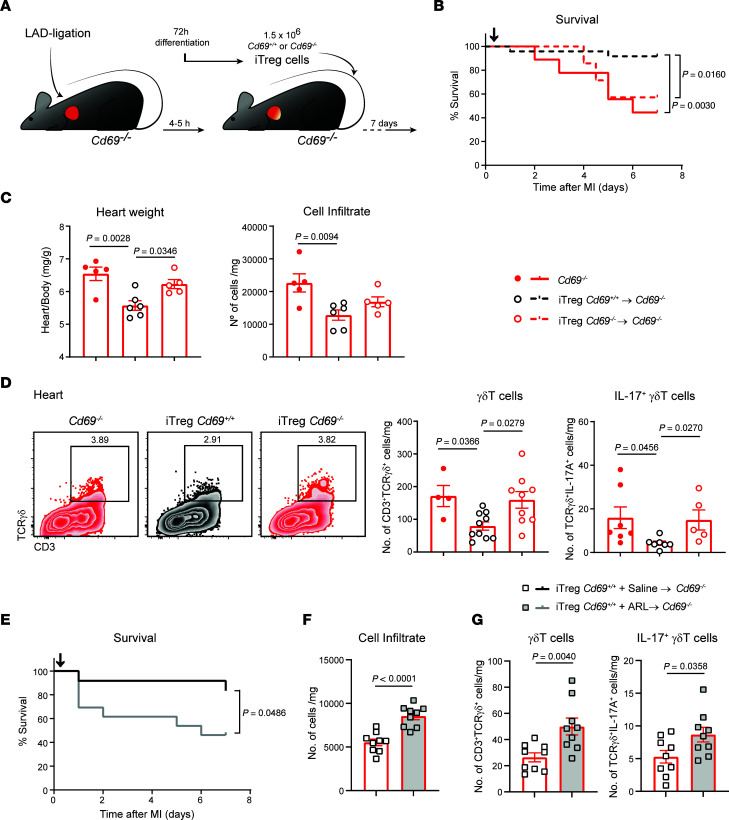
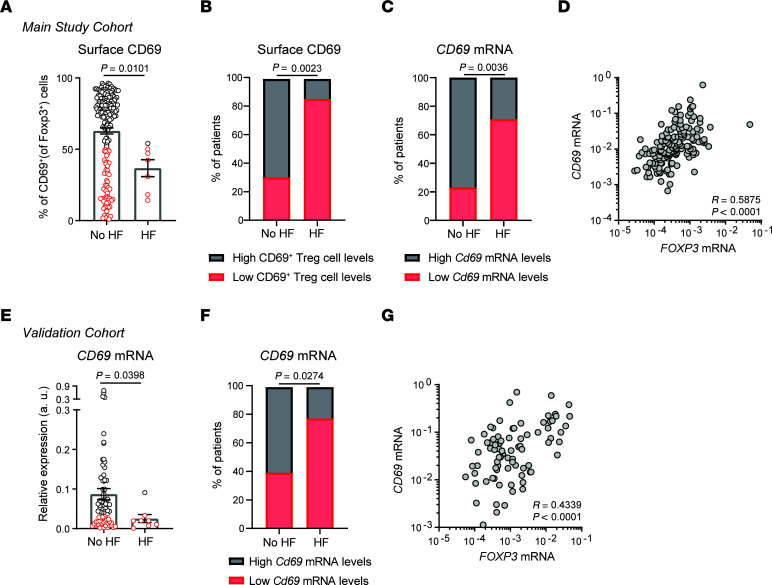
Increasing evidence has pointed to the important function of T cells in controlling immune homeostasis and pathogenesis after myocardial infarction (MI), although the underlying molecular mechanisms remain elusive. In this study, a broad analysis of immune markers in 283 patients revealed significant CD69 overexpression on Tregs after MI. Our results in mice showed that CD69 expression on Tregs increased survival after left anterior descending (LAD) coronary artery ligation. Cd69-/- mice developed strong IL-17+ γδT cell responses after ischemia that increased myocardial inflammation and, consequently, worsened cardiac function. CD69+ Tregs, by induction of AhR-dependent CD39 ectonucleotidase activity, induced apoptosis and decreased IL-17A production in γδT cells. Adoptive transfer of CD69+ Tregs into Cd69-/- mice after LAD ligation reduced IL-17+ γδT cell recruitment, thus increasing survival. Consistently, clinical data from 2 independent cohorts of patients indicated that increased CD69 expression in peripheral blood cells after acute MI was associated with a lower risk of rehospitalization for heart failure (HF) after 2.5 years of follow-up. This result remained significant after adjustment for age, sex, and traditional cardiac damage biomarkers. Our data highlight CD69 expression on Tregs as a potential prognostic factor and a therapeutic option to prevent HF after MI.
Keywords: Cardiology; Cardiovascular disease; Heart failure; Immunology; T cells.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
