

A joint ventricle and WMH segmentation from MRI for evaluation of healthy and pathological changes in the aging brain
- PMID: 36067136
- PMCID: PMC9447923
- DOI: 10.1371/journal.pone.0274212
A joint ventricle and WMH segmentation from MRI for evaluation of healthy and pathological changes in the aging brain
Abstract
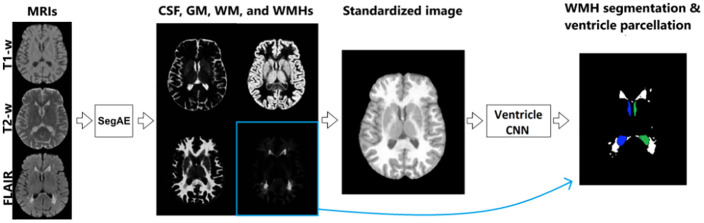
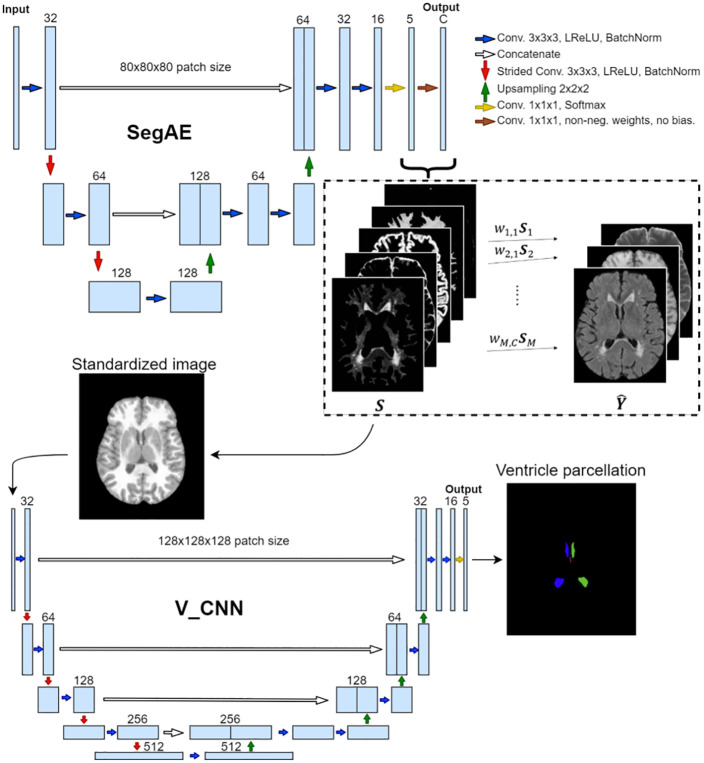
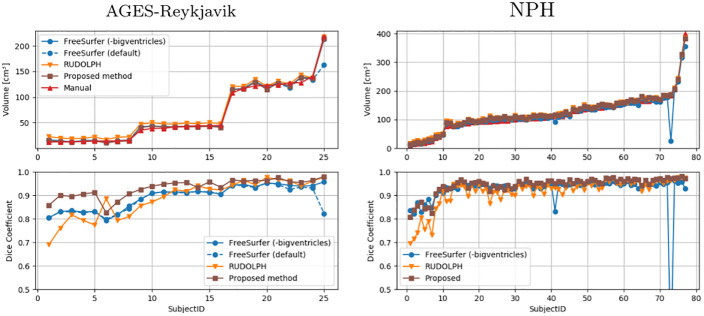
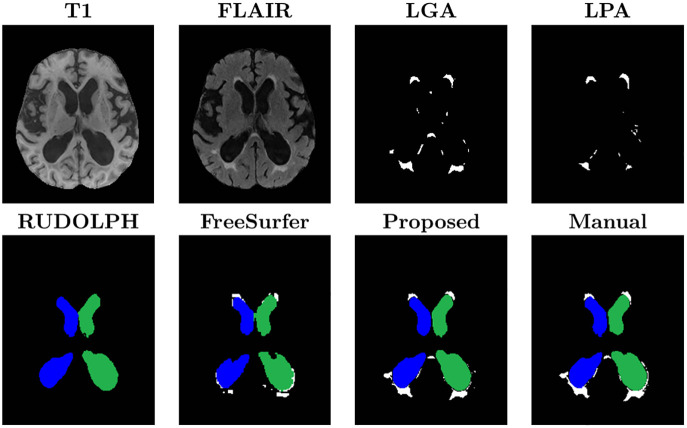
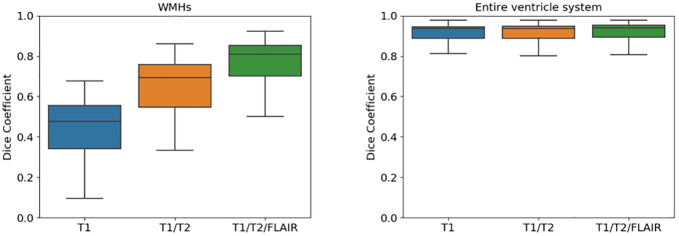
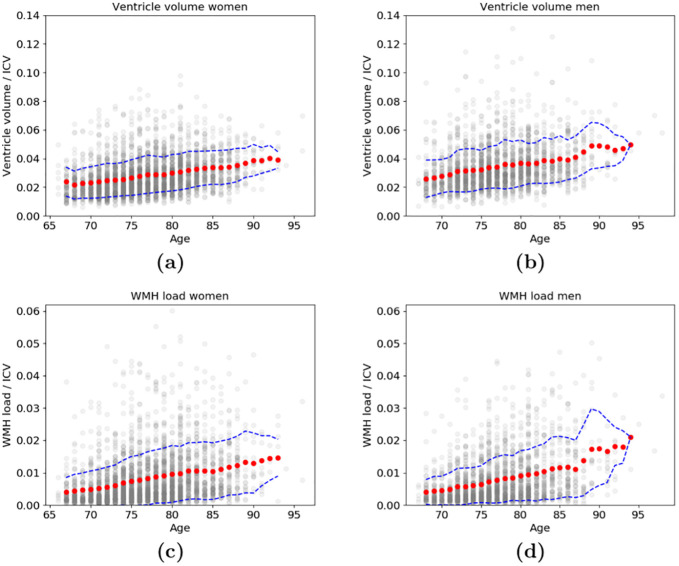
Age-related changes in brain structure include atrophy of the brain parenchyma and white matter changes of presumed vascular origin. Enlargement of the ventricles may occur due to atrophy or impaired cerebrospinal fluid (CSF) circulation. The co-occurrence of these changes in neurodegenerative diseases and in aging brains often requires investigators to take both into account when studying the brain, however, automated segmentation of enlarged ventricles and white matter hyperintensities (WMHs) can be a challenging task. Here, we present a hybrid multi-atlas segmentation and convolutional autoencoder approach for joint ventricle parcellation and WMH segmentation from magnetic resonance images (MRIs). Our fully automated approach uses a convolutional autoencoder to generate a standardized image of grey matter, white matter, CSF, and WMHs, which, in conjunction with labels generated by a multi-atlas segmentation approach, is then fed into a convolutional neural network to parcellate the ventricular system. Hence, our approach does not depend on manually delineated training data for new data sets. The segmentation pipeline was validated on both healthy elderly subjects and subjects with normal pressure hydrocephalus using ground truth manual labels and compared with state-of-the-art segmentation methods. We then applied the method to a cohort of 2401 elderly brains to investigate associations of ventricle volume and WMH load with various demographics and clinical biomarkers, using a multiple regression model. Our results indicate that the ventricle volume and WMH load are both highly variable in a cohort of elderly subjects and there is an independent association between the two, which highlights the importance of taking both the possibility of enlarged ventricles and WMHs into account when studying the aging brain.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
