

Associations between insomnia and pregnancy and perinatal outcomes: Evidence from mendelian randomization and multivariable regression analyses
- PMID: 36067251
- PMCID: PMC9488815
- DOI: 10.1371/journal.pmed.1004090
Associations between insomnia and pregnancy and perinatal outcomes: Evidence from mendelian randomization and multivariable regression analyses
Abstract
Background: Insomnia is common and associated with adverse pregnancy and perinatal outcomes in observational studies. However, those associations could be vulnerable to residual confounding or reverse causality. Our aim was to estimate the association of insomnia with stillbirth, miscarriage, gestational diabetes (GD), hypertensive disorders of pregnancy (HDP), perinatal depression, preterm birth (PTB), and low/high offspring birthweight (LBW/HBW).
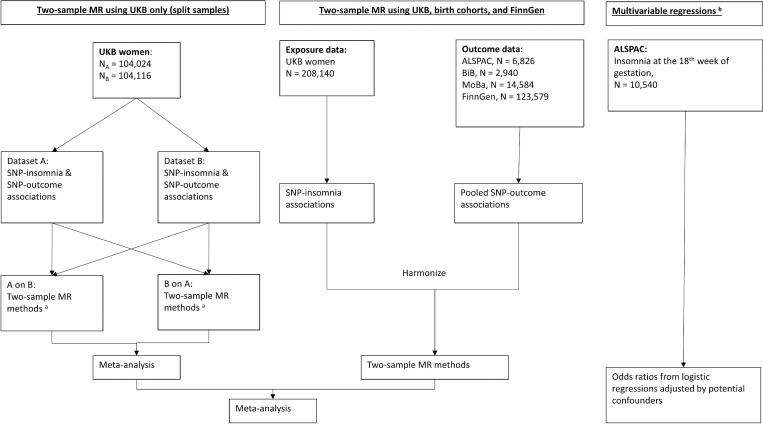
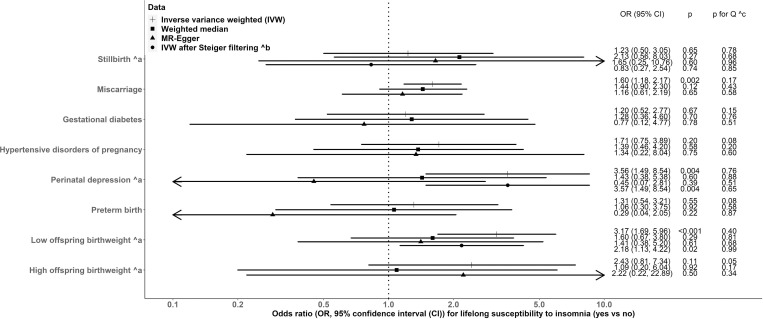
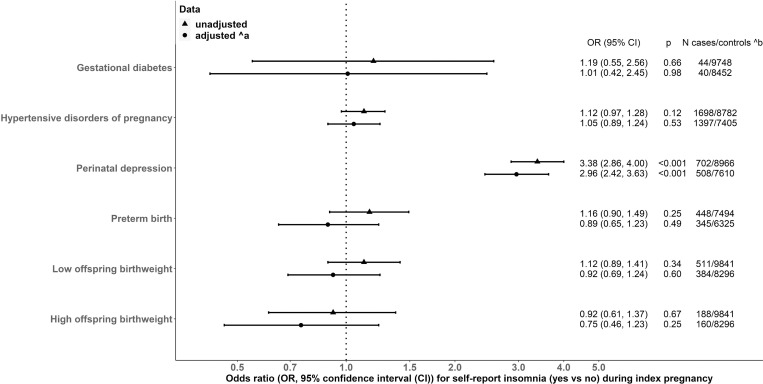
Methods and findings: We used 2-sample mendelian randomization (MR) with 81 single-nucleotide polymorphisms (SNPs) instrumenting for a lifelong predisposition to insomnia. Our outcomes included ever experiencing stillbirth, ever experiencing miscarriage, GD, HDP, perinatal depression, PTB (gestational age <37 completed weeks), LBW (<2,500 grams), and HBW (>4,500 grams). We used data from women of European descent (N = 356,069, mean ages at delivery 25.5 to 30.0 years) from UK Biobank (UKB), FinnGen, Avon Longitudinal Study of Parents and Children (ALSPAC), Born in Bradford (BiB), and the Norwegian Mother, Father and Child Cohort (MoBa). Main MR analyses used inverse variance weighting (IVW), with weighted median and MR-Egger as sensitivity analyses. We compared MR estimates with multivariable regression of insomnia in pregnancy on outcomes in ALSPAC (N = 11,745). IVW showed evidence of an association of genetic susceptibility to insomnia with miscarriage (odds ratio (OR): 1.60, 95% confidence interval (CI): 1.18, 2.17, p = 0.002), perinatal depression (OR 3.56, 95% CI: 1.49, 8.54, p = 0.004), and LBW (OR 3.17, 95% CI: 1.69, 5.96, p < 0.001). IVW results did not support associations of insomnia with stillbirth, GD, HDP, PTB, and HBW, with wide CIs including the null. Associations of genetic susceptibility to insomnia with miscarriage, perinatal depression, and LBW were not observed in weighted median or MR-Egger analyses. Results from these sensitivity analyses were directionally consistent with IVW results for all outcomes, with the exception of GD, perinatal depression, and PTB in MR-Egger. Multivariable regression showed associations of insomnia at 18 weeks of gestation with perinatal depression (OR 2.96, 95% CI: 2.42, 3.63, p < 0.001), but not with LBW (OR 0.92, 95% CI: 0.69, 1.24, p = 0.60). Multivariable regression with miscarriage and stillbirth was not possible due to small numbers in index pregnancies. Key limitations are potential horizontal pleiotropy (particularly for perinatal depression) and low statistical power in MR, and residual confounding in multivariable regression.
Conclusions: In this study, we observed some evidence in support of a possible causal relationship between genetically predicted insomnia and miscarriage, perinatal depression, and LBW. Our study also found observational evidence in support of an association between insomnia in pregnancy and perinatal depression, with no clear multivariable evidence of an association with LBW. Our findings highlight the importance of healthy sleep in women of reproductive age, though replication in larger studies, including with genetic instruments specific to insomnia in pregnancy are important.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: KT has acted as a consultant for CHDI Foundation, and Expert Witness to the High Court in England, called by the UK Medicines and Healthcare products Regulatory Agency, defendants in a case on hormonal pregnancy tests and congenital anomalies 2021/22. DAL has received support from Medtronic LTD and Roche Diagnostics for biomarker research that is not related to the study presented in this paper. The other authors report no conflicts.
Figures
References
Publication types
MeSH terms
Grants and funding
- G0600705/MRC_/Medical Research Council/United Kingdom
- WT088806/WT_/Wellcome Trust/United Kingdom
- CS/16/4/32482/BHF_/British Heart Foundation/United Kingdom
- MC_UU_00011/1/MRC_/Medical Research Council/United Kingdom
- MM_UU_00011/3/MRC_/Medical Research Council/United Kingdom
- MC_PC_21038/MRC_/Medical Research Council/United Kingdom
- NF-SI-0611010196/DH_/Department of Health/United Kingdom
- MC_PC_15018/MRC_/Medical Research Council/United Kingdom
- MC_UU_00011/6/MRC_/Medical Research Council/United Kingdom
- CH/F/20/9003/BHF_/British Heart Foundation/United Kingdom
- NIHR200166/DH_/Department of Health/United Kingdom
- CH/F/20/90003/BHF_/British Heart Foundation/United Kingdom
- MC_PC_17228/MRC_/Medical Research Council/United Kingdom
- MR/N024397/1/MRC_/Medical Research Council/United Kingdom
- FS/17/37/32937/BHF_/British Heart Foundation/United Kingdom
- MC_PC_19009/MRC_/Medical Research Council/United Kingdom
- NF-0616-10102/DH_/Department of Health/United Kingdom
- MC_QA137853/MRC_/Medical Research Council/United Kingdom
- MM_UU_00011/6/MRC_/Medical Research Council/United Kingdom
- 669545/ERC_/European Research Council/International
- MM_UU_00011/1/MRC_/Medical Research Council/United Kingdom
- 217065/Z/19/Z/MRC_/Medical Research Council/United Kingdom
- 947684/ERC_/European Research Council/International
- WT223601/Z/21/Z/WT_/Wellcome Trust/United Kingdom
- 202802/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- WT101597MA/WT_/Wellcome Trust/United Kingdom
- G9815508/MRC_/Medical Research Council/United Kingdom
- MR/P014054/1/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
