

Placenta Accreta Spectrum Prenatal Diagnosis Performance: Are Ultrasound False-positive Results Acceptable in Limited-resources Settings?
- PMID: 36067797
- PMCID: PMC9948072
- DOI: 10.1055/s-0042-1751061
Placenta Accreta Spectrum Prenatal Diagnosis Performance: Are Ultrasound False-positive Results Acceptable in Limited-resources Settings?
Abstract
Objective: The immediate referral of patients with risk factors for placenta accreta spectrum (PAS) to specialized centers is recommended, thus favoring an early diagnosis and an interdisciplinary management. However, diagnostic errors are frequent, even in referral centers (RCs). We sought to evaluate the performance of the prenatal diagnosis for PAS in a Latin American hospital.
Methods: A retrospective descriptive study including patients referred due to the suspicion of PAS was conducted. Data from the prenatal imaging studies were compared with the final diagnoses (intraoperative and/or histological).
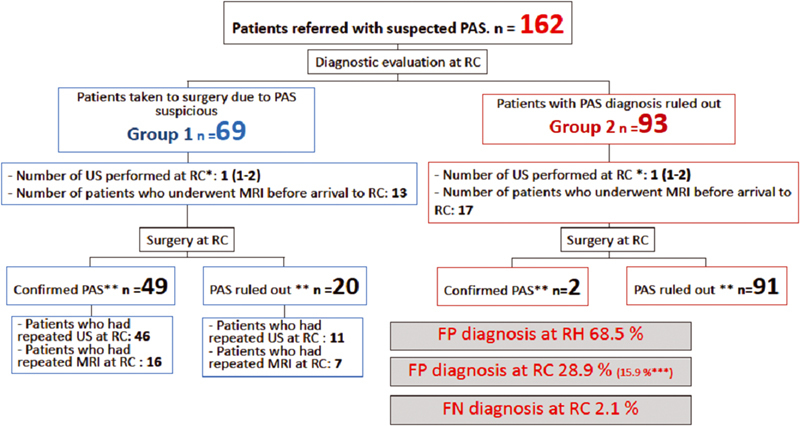
Results: A total of 162 patients were included in the present study. The median gestational age at the time of the first PAS suspicious ultrasound was 29 weeks, but patients arrived at the PAS RC at 34 weeks. The frequency of false-positive results at referring hospitals was 68.5%. Sixty-nine patients underwent surgery based on the suspicion of PAS at 35 weeks, and there was a 28.9% false-positive rate at the RC. In 93 patients, the diagnosis of PAS was ruled out at the RC, with a 2.1% false-negative frequency.
Conclusion: The prenatal diagnosis of PAS is better at the RC. However, even in these centers, false-positive results are common; therefore, the intraoperative confirmation of the diagnosis of PAS is essential.
Objetivo: Recomenda-se o encaminhamento imediato de pacientes com fatores de risco para espectro placentário acreta (PAS, na sigla em inglês) para centros especializados, favorecendo assim o diagnóstico precoce e o manejo interdisciplinar. No entanto, erros diagnósticos são frequentes, mesmo em centros de referência (CRs). Buscou-se avaliar o desempenho do diagnóstico pré-natal para PAS em um hospital latino-americano. MéTODOS: Um estudo descritivo retrospectivo incluindo pacientes encaminhados por suspeita de SAP foi realizado. Os dados dos exames de imagem do pré-natal foram comparados com os diagnósticos finais (intraoperatórios e/ou histológicos).
Resultados: Foram incluídos 162 pacientes no presente estudo. A idade gestacional mediana no momento da primeira ultrassonografia suspeita de PAS foi de 29 semanas, mas as pacientes chegaram ao CR de PAS com 34 semanas. A frequência de resultados falso-positivos nos hospitais de referência foi de 68,5%. Sessenta e nove pacientes foram operadas com base na suspeita de PAS com 35 semanas e houve 28,9% de falso-positivos no CR. Em 93 pacientes, o diagnóstico de PAS foi descartado no CR, com frequência de falso-negativos de 2,1%. CONCLUSãO: O diagnóstico pré-natal de PAS é melhor no CR. Entretanto, mesmo nestes centros, resultados falso-positivos são comuns; portanto, a confirmação intraoperatória do diagnóstico de SAP é essencial.
Federação Brasileira de Ginecologia e Obstetrícia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/).
Conflict of interest statement
The authors have no conflict of interests to declare.
Figures
Similar articles
-
Third-trimester ultrasound for antenatal diagnosis of placenta accreta spectrum in women with placenta previa: results from the ADoPAD study.Ultrasound Obstet Gynecol. 2022 Sep;60(3):381-389. doi: 10.1002/uog.24889. Ultrasound Obstet Gynecol. 2022. PMID: 35247287 Free PMC article.
-
Effectiveness of contingent screening for placenta accreta spectrum disorders based on persistent low-lying placenta and previous uterine surgery.Ultrasound Obstet Gynecol. 2021 Jan;57(1):91-96. doi: 10.1002/uog.23100. Ultrasound Obstet Gynecol. 2021. PMID: 32865834
-
Difficulties in the Management of Placenta Accreta Spectrum in Hospitals with Limited Resources.Rev Bras Ginecol Obstet. 2022 May;44(5):467-474. doi: 10.1055/s-0042-1742408. Epub 2022 Apr 26. Rev Bras Ginecol Obstet. 2022. PMID: 35472821 Free PMC article.
-
Risk factors, histopathology and diagnostic accuracy in posterior placenta accreta spectrum disorders: systematic review and meta-analysis.Ultrasound Obstet Gynecol. 2021 Jun;57(6):903-909. doi: 10.1002/uog.22183. Ultrasound Obstet Gynecol. 2021. PMID: 32840934
-
Diagnostic accuracy of ultrasound in the diagnosis of Placenta accreta spectrum: systematic review and meta-analysis.BMC Pregnancy Childbirth. 2023 May 15;23(1):354. doi: 10.1186/s12884-023-05675-6. BMC Pregnancy Childbirth. 2023. PMID: 37189095 Free PMC article.
Cited by
-
Placenta Accreta Spectrum Disorders: Current Recommendations from the Perspective of Antenatal Imaging.Rev Bras Ginecol Obstet. 2023 Jun;45(6):297-302. doi: 10.1055/s-0043-1770917. Epub 2023 Jul 21. Rev Bras Ginecol Obstet. 2023. PMID: 37494571 Free PMC article. No abstract available.
References
-
- Maternal Death Exploratory Committee in Japan and the Japan Association of Obstetricians and Gynecologists . Hasegawa J, Tanaka H, Katsuragi S, Sekizawa A, Ishiwata I, Ikeda T. Maternal deaths in Japan due to abnormally invasive placenta. Int J Gynaecol Obstet. 2018;140(03):375–376. doi: 10.1002/ijgo.12368. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources