

Renal outcomes according to renal replacement therapy modality and treatment protocol in the ATN and RENAL trials
- PMID: 36068554
- PMCID: PMC9450407
- DOI: 10.1186/s13054-022-04151-5
Renal outcomes according to renal replacement therapy modality and treatment protocol in the ATN and RENAL trials
Abstract
Background: In critically ill patients with acute kidney injury, renal replacement therapy (RRT) modality and treatment protocols may affect kidney recovery. This study explored whether RRT modality and treatment protocol affected RRT dependence in the 'Randomized Evaluation of Normal versus Augmented Level of RRT' and the 'Acute Renal Failure Trial Network' (ATN) trials.
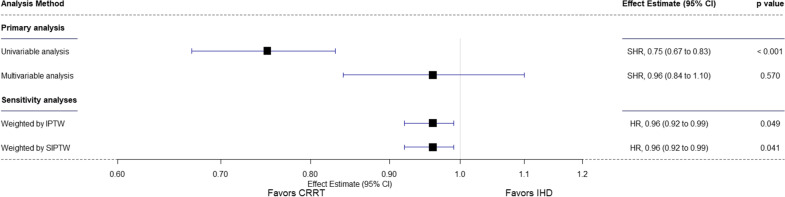
Methods: Primary outcome was 28-day RRT dependence. Secondary outcomes included RRT dependence among survivors and in different SOFA-based treatment protocol groups. We used the Fine-Gray competing-risk model sub-distribution hazard ratio (SHR) to assess the primary outcome. Analyses were adjusted for confounders.
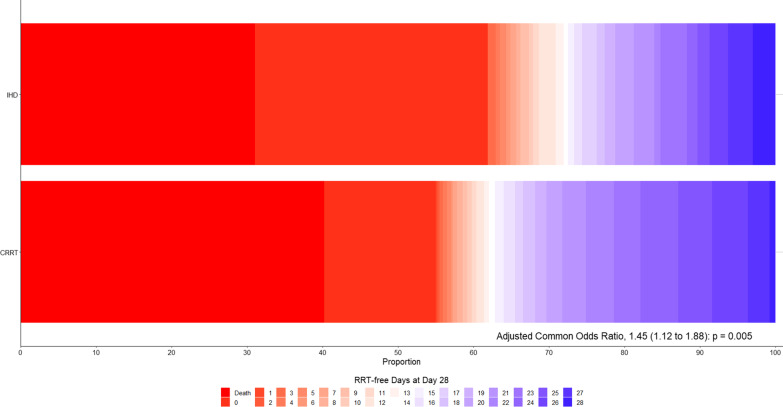
Results: Of 2542 patients, 2175 (85.5%) received continuous RRT (CRRT) and 367 (14.4%) received intermittent hemodialysis (IHD) as first RRT modality. CRRT-first patients had greater illness severity. After adjustment, there was no between-group difference in 28-day RRT dependence (SHR, 0.96 [95% CI 0.84-1.10]; p = 0.570) or hospital mortality (odds ratio [OR], 1.14 [95% CI 0.86-1.52]; p = 0.361) However, among survivors, CRRT-first was associated with decreased 28-day RRT dependence (OR, 0.54 [95% CI 0.37-0.80]; p = 0.002) and more RRT-free days (common OR: 1.38 [95% CI 1.11-1.71]). Moreover, among CRRT-first patient, the ATN treatment protocol was associated with fewer RRT-free days, greater mortality, and a fourfold increase in RRT dependence at day 28.
Conclusions: There was no difference in RRT dependence at day 28 between IHD and CRRT. However, among survivors and after adjustment, both IHD-first and the ATN treatment protocol were strongly associated with greater risk of RRT dependence at 28 days after randomization. Trial registration NCT00221013 registered September 22, 2005, and NCT00076219 registered January 19, 2004.
Keywords: Acute kidney injury; Continuous renal replacement therapy; Dialysis dependence; Intermittent hemodialysis; Mortality.
© 2022. The Author(s).
Conflict of interest statement
Dr Serpa Neto reported receiving grants and personal fees from Dräger, outside the submitted work. Dr Bellomo reported receiving grants from Baxter International outside the submitted work. Dr Naorungroj declared that they have no relevant financial interests. Dr Amanda Y Wang is supported by RACP Jacquot Research Establishment Fellowship, Australia.
Figures


References
-
- Johansen KL, Smith MW, Unruh ML, Siroka AM, O'Connor TZ, Palevsky PM. Predictors of health utility among 60-day survivors of acute kidney injury in the Veterans Affairs/National Institutes of Health Acute Renal Failure Trial Network Study. Clin J Am Soc Nephrol. 2010;5(8):1366–1372. doi: 10.2215/CJN.02570310. - DOI - PMC - PubMed
-
- Kidney Disease Improving Global Outcomes (KDIGO) AKI Working Group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2:1–138.
-
- Lins RL, Elseviers MM, Van der Niepen P, Hoste E, Malbrain ML, Damas P, et al. Intermittent versus continuous renal replacement therapy for acute kidney injury patients admitted to the intensive care unit: results of a randomized clinical trial. Nephrol Dial Transpl. 2009;24(2):512–518. doi: 10.1093/ndt/gfn560. - DOI - PubMed
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
