

The effect of immunosuppressive therapy on cardiac involvements in anti-mitochondrial antibody-positive myositis
- PMID: 36068648
- PMCID: PMC9773721
- DOI: 10.1002/ehf2.14138
The effect of immunosuppressive therapy on cardiac involvements in anti-mitochondrial antibody-positive myositis
Abstract
Aims: Anti-mitochondrial antibody (AMA)-positive myositis is frequently associated with various cardiac involvements, such as arrhythmia and left ventricular (LV) dysfunction. However, the efficacy of immunosuppressive therapy in these complications remains unknown. This study aimed to investigate the cardiac response to immunosuppressive therapy in patients with AMA-positive myositis.
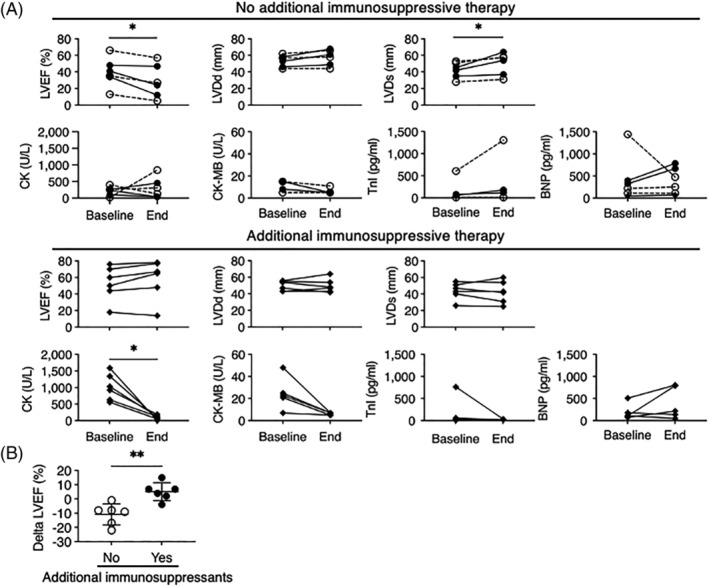
Methods and results: The clinical data of 15 AMA-positive myositis patients with cardiac involvement were retrospectively collected at our centre. To evaluate the effects of immunosuppressive therapy, echocardiographic and laboratory data of patients who received glucocorticoid therapy with additional immunosuppressants (n = 6) and those who did not (n = 6) were compared. Also, the characteristics of patients with or without >5% LV ejection fraction (LVEF) decline during the follow-up period (n = 5 vs. n = 7) were compared. Thirteen patients (87%) had arrhythmias, and eight patients (53%) had LV wall motion abnormalities. Although arrhythmias decreased after treatment, reduced LVEF and LV wall motion abnormalities persisted. Further investigation revealed an increased LV end-systolic dimension and reduced LVEF in patients without additional immunosuppressive therapy, while those in patients with additional immunosuppressive therapy were maintained. Six of seven patients (86%) without LVEF decline received additional immunosuppressive therapy, whereas no patients with LVEF decline had additional immunosuppressive therapy.
Conclusions: Cardiac involvement in AMA-positive myositis may worsen even with glucocorticoid monotherapy, and there might be some associations between the change of LV function and additional immunosuppressive therapy.
Keywords: Anti-mitochondrial antibody; Cardiac involvement; Immunosuppressive therapy; Myositis.
© 2022 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
EA belongs to the Department, endowed by NIPRO‐Corp, Terumo‐Corp., Senko Medical‐Instrument‐Mfg., Century‐Medical, Inc., ONO‐pharmaceutical‐Co., Ltd. Medtronic‐JAPAN Co., Ltd, Nippon‐Shinyaku Co., Ltd, Mochida Pharmaceutical Co.; Boehringer Ingelheim Pharmaceuticals Inc., Abiomed‐Inc, AQuA‐Inc, Fukuda‐Denshi Co., Ltd, and Sun‐Medical‐Technology‐Research Corp.
Figures

References
-
- Tschöpe C, Ammirati E, Bozkurt B, Caforio ALP, Cooper LT, Felix SB, Hare JM, Heidecker B, Heymans S, Hübner N, Kelle S, Klingel K, Maatz H, Parwani AS, Spillmann F, Starling RC, Tsutsui H, Seferovic P, Van Linthout S. Myocarditis and inflammatory cardiomyopathy: Current evidence and future directions. Nat Rev Cardiol. 2021; 18: 169–193. - PMC - PubMed
-
- Mavrogeni S, Bratis K, Karabela G, Stavropoulos E, Sfendouraki E, Kolovou G. Myocarditis during acute inflammatory myopathies: Evaluation using clinical criteria and cardiac magnetic resonance imaging. Int J Cardiol. 2013; 164: e3–e4. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
